
Long-term treatment of neovascular age-related macular degeneration (nAMD) is placing an increasing burden on patients, their carers, practitioners, and government resources. This article explores promising treatments on the horizon.
The phrase “age-related macular degeneration is the leading cause of blindness in the western world” has appeared in many research grant applications. The statement holds true and is not surprising, given that the burden of its treatment is now being felt worldwide. In the United Kingdom, ophthalmology outpatient attendance is the highest among all the specialties. It has overtaken orthopaedic outpatient attendance numbers since 2017, with nearly eight million attendance episodes in the year 2019-2020.1 Undoubtedly, the increasing number of patients receiving treatment for nAMD contributes to this figure and leads to a tremendous drain on the National Health Service resource. In Australia, the two anti-VEGF drugs for nAMD are in the top 10 most costly drugs prescribed, Aflibercept (Eylea) topped the list as the number one most costly Pharmaceutical Benefits Scheme (PBS)/Repatriation Pharmaceutical Benefits Scheme (RPBS) drug to government, not including rebates, in 2019-2020.2 A total of 315,200 prescriptions for aflibercept cost the government nearly AU$400 million. The seventh most costly PBS/RPBS drug to the government was Ranibizumab (Lucentis), and it cost the taxpayer $218 million for 190,126 prescriptions in the same period.
In Australia, the two anti-vascular endothelial growth factor (anti-VEGF) drugs for nAMD are in the top 10 most costly drugs prescribed

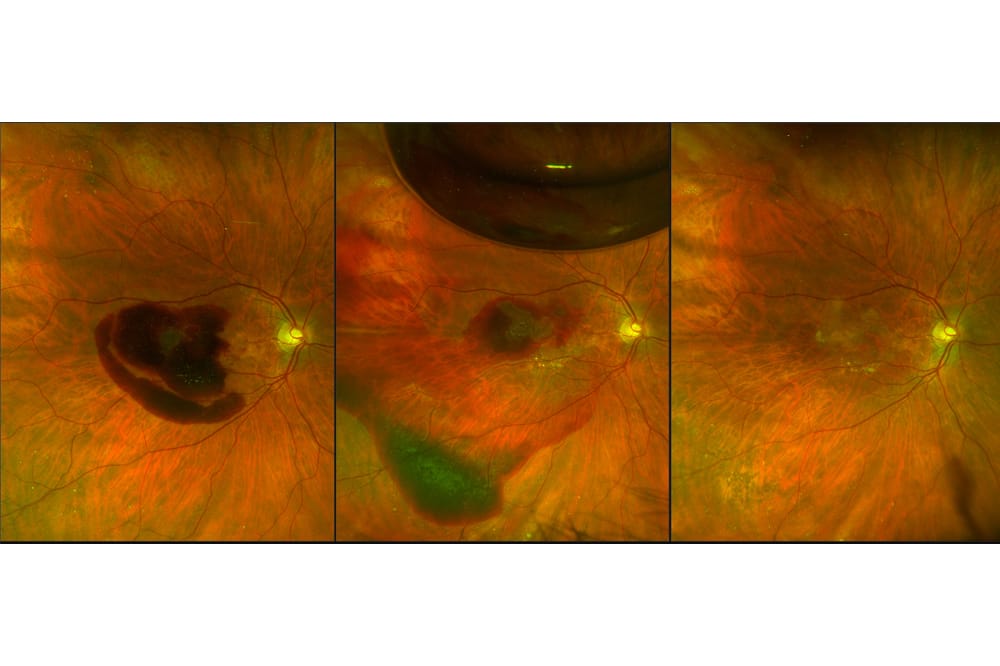
Figure 1. (A) A 69-year-old woman who was undertreated for nAMD in the right eye resulting in a large submacular haemorrhage; (B) She had pneumatic displacement of the blood via intravitreal C3F8 gas injection, (C) Her best corrected visual acuity in this eye returned to 6/9 nine months later.
A recent study confirmed that this treatment burden is not getting any lighter: not only were the number of patients requiring treatment increasing, but those who were undertreated had a poorer prognosis than those who were treated more frequently (Figure 1).3 Visual outcomes were better in eyes from an area where more injections were delivered using a treat and extend regimen. It is imperative that a safe, sustainable, economical, and effective treatment can be found for both dry AMD and nAMD.
WHAT’S ON THE HORIZON IN THE TREATMENT OF NAMD?
Biosimilars
Existing anti-VEGF agents, including Bevacizumab (targeting VEGF A), Ranibizumab (targeting VEGF A), and Aflibercept (targeting VEGF A, B, Placental Growth Factor [PIGF]), have been highly effective and transformed the treatment of nAMD. However, the costs of these drugs are still high, and the financial burden is enormous for many individuals, insurance companies, and countries. These drugs have been around for several years, and their patents are running out. Pharmaceutical companies can create drugs similar enough to proven biotherapeutics in safety and efficacy, but at a lower cost. Here is where biosimilars come in. Biosimilars are not generic; they may be made from different cell lines and may have other inflammatory properties. A 2020 study found 25 ophthalmic biosimilars in development: four for aflibercept, eight for bevacizumab, six for ranibizumab, and seven for adalimumab.4 As with any pharmaceutical products, biosimilars will have to clear a series of hurdles (from study design to assessments of safety and efficacy, cost issues, and offlabel use) before they achieve broad-based acceptance by clinicians. There are currently several clinical studies/trials assessing these agents, and one day they may provide more economically viable alternatives to currently approved anti-VEGF agents.
Newer Agents With Longer Durability
The efficacy of Brolucizumab (targeting VEGF A) is promising, but there are on-going concerns with inflammatory adverse events (especially vasculitis). It has the Food and Drug Administration (FDA) approval in the USA, but it is still awaiting approval in Australia. Abicipar pegol is designed in a DARPins (designed ankyrin repeat proteins) format; despite the results of its encouraging trial, regulatory approval is not forthcoming, also due to its inflammatory properties.5 Conbercept has a high affinity to all VEGF A isoforms, B, C and PIGF. It is being used in China and is undergoing clinical trials in the USA and elsewhere; full results are expected soon.

Figure 2. Schematic diagrams showing different methods of gene therapy delivery. (A) Subretinal delivery via vitrectomy, (B) In office intravitreal injection, (C) Subretinal delivery via suprachoroidal injection.10
Currently, approved anti-VEGF agents target VEGF A primarily; this can result in up-regulation of VEGF C in the treated eye. OPT-302, a new agent that blocks VEGF C, is combined with anti-VEGF A agents in clinical trials as a treatment that may potentiate their therapeutic effects. OPT-302 recently completed its phase 2b trial and met its primary endpoints. The Phase 3 trials, referred to as ShORe and COAST, will be double-masked, sham-controlled trials that enrol treatment-naïve patients and assess the efficacy and safety of 2.0mg OPT-302 in combination with anti-VEGF-A therapy, compared to standard of care anti-VEGF-A monotherapy. Patients will continue to be dosed until week 96 to further assess longterm safety at week 100.6,7
KSI-301 is an antibody biopolymer conjugate (ABC). At the molecular level, anti-VEGF A complementary-determining regions (CDR) are placed on an IgG antibody, covalently linked to a phosphorylcholine polymer. This biopolymer matrix is a large molecule; hence it has a longer half-life and can deliver a higher molar concentration, resulting in longer intraocular durability than existing drugs. The results of a phase 1b study in nAMD, with loading doses with a capped, as required, treatment every six months, showed 5.8 letters gain over 44 weeks with 1.32 mean injections over the study period. The phase 2b/3 trial, DAZZLE, had three loading doses followed by individualised dosing of 12, 16, or 20 weeks. Meanwhile, other variants of this biopolymer conjugate are being developed, including KSI-501 (anti-VEGF, Interleukin-6 dual inhibitor) and KSI-601 (triplet inhibitor for dry AMD).6,7
Faricimab is the first investigational bispecific antibody designed for the eye. It targets two distinct pathways – via angiopoietin-2 (Ang-2) and VEGF A. Two phase 3 studies, TENAYA and LUCERNE, met their primary endpoint and showed that eyes receiving Faricimab injections at fixed intervals of up to every 16 weeks achieved visual acuity outcomes that were non-inferior to those receiving aflibercept injections every eight weeks. Further studies are underway.6,7
Recently, a novel agent, EXN 407, has been developed to inhibit production of VEGF A through selective inhibition of serine/threonine-protein kinase 1 (SRPK1)- mediated VEGF splicing. These inhibitors have already demonstrated superior efficacy as topical agents in preclinical models of neovascularisation.22 Phase 1b/2 clinical trial for its use in diabetic macular oedema is underway. This topical agent may be a candidate for future treatment of nCNV.

Figure 3. A schematic diagram showing the different pathways of the complement system and the locations where the complement factors act.
Sustained Release Delivery System
Another way to prolong an existing drug’s action is to deliver it slowly over a long period via a refillable reservoir. A permanent, refillable intraocular implant with a customised formulation of ranibizumab has been developed. This port delivery system (PDS) is an implant that is surgically placed at the pars plana in the operating theatre and is refilled via an outpatient (in office) procedure. It is the first surgical treatment for nAMD since submacular surgery and macular translocation. The result of the phase 3 Archway Trial of the PDS with Ranibizumab, with mandated refill exchanges every 24 weeks, is positive and non-inferior to four-weekly Ranibizumab injections. Of PDS treated patients, 98% did not receive additional treatment during the first refill-exchange interval, with a median time of 15.8 months before the need to refill. The adverse event of vitreous haemorrhage, noted early in the phase 2 trial, was addressed by modifying the surgical technique. The main concerns were conjunctival erosion and retraction (2%) and endophthalmitis (up to 1.6%). The Patient Preference Questionnaire that was used in the PDS study showed “93% of patients indicated a strong, or fairly strong preference for PDS”. This treatment can potentially prevent under-treatment. If this is combined with a home monitoring system (e.g. a home optical coherence tomography [OCT] device), it may prolong the need for re-treatment for an extended time.8
Gene Therapy
The most exciting development in the treatment for nAMD is gene therapy. Depending on the disease or genetic defect, the therapeutic effect of gene therapy is achieved by replacing a missing gene, suppressing a defective gene, or artificially introducing a gene into another organism (transgene) to produce the desired protein. In this last method, the viral vector carries the gene of interest into the host cell. The host cell expresses the gene, which is translated into a protein therapeutic product. The gene therapy in nAMD trials is used to produce a VEGF inhibitor in the treated eye, thus creating a de novo anti-VEGF ‘factory’. Substantial reduction in annualised anti- VEGF injection frequency after treatment is expected following this kind of intervention.9
In the phase 1/2a RGX-314 study for previously treated nAMD patients, using an AAV8 vector, a transgene (encoding for a monoclonal antibody fragment similar to Ranibizumab) is inserted via a subretinal injection.10 This method uses an automated microlitre injection – a specialised injection kit with fine foot pedal control for precise microlitre dosing during the vitrectomy procedure. The advantage of this delivery method is that neutralising antibodies don’t generally impact the efficacy of transduction when the gene therapy is delivered into the immune privileged subretinal space. The main drawback is the need for a vitrectomy operation to deliver the gene subretinally. A phase 3 trial is on-going, with the use of a proprietary in-office suprachoroidal injection needle for gene delivery. The surgical technique of suprachoroidal to subretinal delivery is achieved via a sclerostomy where a microcannula is introduced into the subretinal space. A microneedle, through the microcannula, is used to create a saline bleb before the gene therapy is delivered, thus avoiding the need for vitrectomy9 (Figure 2). In August 2020, the FDA granted clearance for this proprietary device, Orbit Subretinal Delivery System (Orbit SDS).

Figure 4. (A) Colour photo of the right eye in a 75-year-old man with BCVA of 6/7.5 showing geographic atrophy, (B) The autofluorescence image of the same eye showed extensive loss of autofluorescence, (C) Raster high definition OCT scan of the macula, showing the proximity of the loss of retinal pigment epithelial cells and their corresponding photoreceptors to the fovea.
Another nAMD gene therapy, ADVM- 022, can be administered via intravitreal injection. The transgene encodes for aflibercept and it employs an AAV.7m8 capsid. The target retinal cells will express aflibercept.10 The OPTIC Study, a phase 1 study, is a two-year multicentre doseranging study, on previously treated nAMD patients with efficacy assessment at 24 and 52 weeks. A phase 3 trial is on-going. Durability is seen out to 92 weeks from a single injection with zero supplemental injections in cohort one. Results to date showed that best corrected visual acuity and central subfield thickness are maintained. There are some signs of low-grade inflammation in treated patients, but it appears to be controllable with topical steroids.9
WHAT’S ON THE HORIZON FOR DRY AMD?
Modifying The Complement System
The most exciting development for treating dry AMD involves modulating the complement system within the eye (Figure 3), or precisely, the different complement factors (CF).12,17 Complement over-activation has been strongly correlated with the development and progression of AMD. There is a clear genetic link between complement and AMD. In individuals homozygous for the risk allele, the likelihood of AMD is increased by a factor of 7.4.20 The initial failure of the complement inhibition pathway in dry AMD treatment did not deter investigators (e.g. Lampalizumab targeting CFD). Recent trials in the complement inhibition pathway (e.g. the inhibition of C3, C5, CFH) produced some promising results in slowing the development of geographic atrophy (GA) (Figure 4A-C).12
In the FILLY study (phase 2 GA study, using a C3 inhibitor APL-2, Pegcetacoplan), APL-2 was administered as an intravitreal injection in the study eye monthly, or every other month, for 12 months, followed by six months of monitoring after the end of treatment. The FILLY trial involves 246 patients at 40 clinical sites in the United States, Australia and New Zealand. The primary endpoint of FILLY was the change in GA lesion size from baseline to month 12 in the treatment group compared to sham. APL-2 administered monthly via intravitreal injection showed a 29% (p=0.008) reduction in GA lesion growth rate compared to sham after 12 months of treatment. With every other monthly administration of APL-2, a 20% (p=0.067) reduction was observed compared to sham. Statistical significance was defined as p<0.1 for this study. However, the choroidal neovascular membrane (CNV) development rates were 21% in patients on monthly treatment and 9% on two-monthly treatment, compared to Sham 1.2%.13 Dose-related higher rates of CNV in treated eyes is a concern and is being further investigated. In a post hoc analysis, the data showed a 39% reduction in the progression rate from nascent GA, an earlier form of the disease, to GA in patients treated with APL-2 monthly versus sham injections, demonstrating that intravitreal APL-2 may slow early disease progression (Euretina Oct 2020).14 Phase 3 trials (DERBY and OAKS) have completed enrolment in July 2020, and top-line results are expected in late 2021.
Another complement inhibitor, Avacincaptad Pegol (Zimura) – a novel C5 inhibitor – was studied in GATHER 1 (a Phase 2/3 study). It was found that monthly doses of 2mg and 4mg of avacincaptad resulted in a reduction of 27% to 28% in geographic atrophy growth rate. This reduction was statistically significant (P = .007 and P = .005 for the two doses, respectively) at the primary endpoint of 12 months, and subsequent follow-up showed an increasing magnitude of effect through 18 months.15 Higher rates of CNV were detected in avacincaptad-treated eyes in GATHER 1. However, the differences in CNV rates between the sham arm and the avacincaptad monthly dose arms were lower than those reported for monthly APL-2. A phase 3 trial (GATHER 2) is on-going.
Complement Factor H (CFH) inhibits the alternative pathway of the complement cascade by blocking the formation of the C3 convertase and assisting in the cleavage of C3b. While it is genetically implicated in about 40% of patients with dry AMD,20 a key therapeutic challenge involves producing CFH and preserving it in vivo. GEM103, a recombinantly produced full-length human factor H protein (rCFH), is being studied in a phase 2 ReGAtta dose-escalation trial in dry AMD patients with CFH loss-offunction gene variants. It is delivered via intravitreal injection. The trial is designed to evaluate safety, tolerability, intraocular pharmacokinetics (PK), and diseaserelevant biomarkers to inform the late-stage development program. The enrolment is completed, and we await the results.16
Gene Therapy
Gene therapy using the complement system is also being investigated. The two main targets are CD59 protein and CFI.
CD59 is a protective protein that is typically found on the plasma membrane of cells. It protects against cell lysis by blocking the formation of a pore known as the membrane attack complex (MAC), which causes ion influx and subsequent osmotic rupture. Studies have shown that patients with AMD have less CD59 present in the retina to protect their cells from damage caused by the complement system. An AAV2 gene therapy called AAVCAGsCD59 (HMR59) is delivered via intravitreal injection.17,18 Since the transgene product is a soluble form of the membrane-bound CD59, it provides the same mode of action as membrane-bound CD59 in vivo: by preventing C5b-8 from combining with C9, MAC formation is unable to occur and cell lysis is inhibited. A phase 2 study is planned for 2021.
The CFI protein regulates the activity of the complement system by cleaving C3b and C4b to prevent the downstream inflammatory effects of the complement cascade. Therefore, it is believed that increasing CFI production could ultimately reduce complement system overactivity and reduce inflammation. Genetic variants exist in patients who are low in CFI. GT005 is an investigational one-time AAV-based gene therapy designed to restore balance to an overactive complement system by increasing CFI production.17,18 In the initial doseescalation phase 1/2 study, FOCUS, which is now complete, patients were treated using a subretinal injection involving vitrectomy and retinotomy. GT005 is being evaluated in two phase 2 clinical trials, EXPLORE and HORIZON, multicentre, randomised controlled trials evaluating the safety and effectiveness of GT005 administered as a single subretinal injection. The trial has been expanded to include additional cohorts, including a dose-expansion cohort and two cohorts in which the Orbit SDS will be used to deliver GT005. EXPLORE is enrolling people who have GA secondary to AMD, who have rare variants in their CFI gene. HORIZON is enrolling a broader group of people who have GA secondary to AMD. The primary endpoint for both trials is the rate of progression of GA over 48 weeks.
THE FUTURE IS BRIGHT
The long-term impact of regular anti- VEGF treatment in nAMD cannot be understated and its benefits can be clearly seen.3 Under-treatment may result in loss of vision. Biosimilars can bring down the cost of treatment, and a number of potential new treatments and modes of delivery that can prolong the efficacy of treatment are in the pipeline. A selection of new agents was discussed in this article, but the list is not meant to be exhaustive.19 There are many hurdles ahead for gene therapy before it becomes a safe and acceptable treatment, but the signs are promising. Going from numerous regular injections to potentially a single treatment utilising gene therapy, with the supplemental rescue injection if needed, is a very transformative and novel concept. This may be the next game changer in the fight against nAMD.
It is also reassuring to know that central macular atrophy does not develop universally in eyes on long-term treatment, as previously feared.3 For dry AMD, we may soon be able to use complement inhibitors in early AMD before developing GA. GA is the main limitation of vision in the medium and longterm, as observed from the Seven-up study,20 and although there may be an increased risk of CNV with these new treatments, there are already many effective treatments for the latter condition. I believe that the imminent future holds the next exciting phase in the war against AMD. With the advent of these new pharmaceutical therapies, this future is bright, and this future is here.
Associate Professor Anthony Kwan undertook his medical training in the United Kingdom and ophthalmology training at Moorfields Eye Hospital in London. He obtained a postgraduate research doctorate (MD) from the University of London in retinal transplantation. He was fellowship trained at the Lions Eye Institute, Perth, and at Moorfields Eye Hospital. A/Prof Kwan is the immediate past chair of the Australian and New Zealand Society of Retinal Specialists (ANZSRS). He is the Director of Queensland Electrodiagnostic and Imaging Centre (QEDIC) and has been the Director of Vitreoretinal Surgery at the Queensland Eye Institute since 2007. He holds the academic title of Associate Professor of Ophthalmology from the University of Queensland and is currently the chair of the research committee of the Macular Disease Foundation Australia.
References
- Hospital Outpatient Activity – NHS Digital (https://digital. nhs.uk/data-and-information/publications/statistical/ hospital-outpatient-activity)
- Top 10 drugs 2019–20 NPS Medicinewise (www.nps.org. au/australian-prescriber/articles/top-10-drugs-2019-20)
- Gillies M, Arnold J, Bhandari S, et al. Ten-year outcomes of neovascular age-related macular degeneration from two regions. Am J Ophthalmol. 2020;210:116-124
- Sharma A, Kumar N, Kuppermann BD, et al. Understanding biosimilars and its regulatory aspects across the globe: an ophthalmology perspective. Br J Ophthalmol 2020;104:2-7.
- Campa C. New Anti-VEGF Drugs in Ophthalmology. Curr Drug Targets. 2020;21(12):1194-1200
- Samanta A, Aziz AA, Jhingan M, et al.. Emerging Therapies in Neovascular Age-Related Macular Degeneration in 2020. Asia Pac J Ophthalmol (Phila). 2020;9(3):250-259.
- Al-Khersan H, Hussain RM, Ciulla TA, et al. Innovative therapies for neovascular age-related macular degeneration. Expert Opin Pharmacother. 2019;20(15):1879-1891
- Chen ER, Kaiser PK. Therapeutic Potential of the Ranibizumab Port Delivery System in the Treatment of AMD: Evidence to Date. Clin Ophthalmol. 2020;19(14):1349-1355.
- Guimaraes TAC, Georgiou M, Bainbridge JWB, et al. Gene therapy for neovascular age-related macular degeneration: rationale, clinical trials and future directions. Br J Ophthalmol. 2021;105(2):151-157.
- Khanani AM, Holekamp N, Boyer D, et al. Gene Therapy: An Emerging Frontier in the Treatment of Neovascular Diseases. Retina Today 2020 Apr; Supplement. (https:// retinatoday.com/pdfs/0420_supp2.pdf)
- Guimaraes TAC, Georgiou M, Bainbridge JWB, Michaelides M. Gene therapy for neovascular age-related macular degeneration: rationale, clinical trials and future directions. Br J Ophthalmol. 2021 Feb;105(2):151-157. doi: 10.1136/bjophthalmol-2020-316195. Epub 2020 Apr 8. PMID: 32269060; PMCID: PMC7848059.
- Ammar MJ, Hsu J, Chiang A, et al. Age-related macular degeneration therapy: a review. Curr Opin Ophthalmol. 2020;31(3):215-221.
13 Allen Chiang, David Lally; Assessment of Progression of Geographic Atrophy in the FILLY Study. Invest Ophthalmol Vis Sci 2020;61(7):4307.
- Sadda S. Impact of Pegcetacoplan on Progression of Nascent Atrophy in AMD. Euretina Virtual Conference 2020. (www.euretina.org/congress/amsterdam-2020/ schedule/?type=EURETINA-Session)
- Jaffe GJ, Westby K, Csaky KG, et al. C5 Inhibitor Avacincaptad Pegol for Geographic Atrophy Due to Age- Related Macular Degeneration: A Randomised Pivotal Phase 2/3 Trial. Ophthalmology. 2020:S0161-6420(20)30845-9.
- A Multiple Dose Study of Repeat Intravitreal Injections of GEM103 in Dry Age-related Macular Degeneration (www. clinicaltrials.gov/ct2/show/NCT04643886)
- Kassa E, Ciulla TA, Hussain RM, Dugel PU. Complement inhibition as a therapeutic strategy in retinal disorders. Expert Opin Biol Ther. 2019;19(4):335-342.
- Akyol E, Lotery A. Gene, Cell and Antibody-Based Therapies for the Treatment of Age-Related Macular Degeneration. Biologics. 2020;14:83-94.
- Kaiser PK. Retina Pipeline: A View Into Ongoing Innovation [Interactive Pipeline]. Retina Today. Digital Supplement. 2021. (https://retinatoday.com/resource/ therapeutic-pipeline-for-amd)
- Rofagha S, Bhisitkul RB, Boyer DS, et al. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: A multicenter cohort study (SEVENUP). Ophthalmology. 2013;120:2292-2299
- Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science. 2005;308(5720):385-9.
- EXN407, a novel topical therapeutic candidate with high retinal bioavailability for the treatment of diabetic macular oedema, inhibits ocular neovascularisation. Batson J, Toop H, Liddell S, et al. Invest Ophth Vis Sci 2019, 60: 26 (meeting abstract).





