

Small aperture technology, leveraged by the IC-8 intraocular lens (IOL), can provide patients with complex corneas – who are not always candidates for traditional IOL technology – a premium outcome. The pinhole optic-based implants fill a much-needed gap for the more than 10% of cataract patients presenting with irregularities.
As a surgeon who specialises in cataract surgery for patients with complex corneas – those with ocular histories or corneal shapes that can make treatment at the time of cataract surgery complex – the prevalence of irregular astigmatism in my clinic is anywhere from 30% to 40%. Most of these individuals have had a previous corneal transplant or refractive surgery, commonly LASIK and less often, radial keratotomy. Some have corneal scars due to a previous infection, such as herpes simplex, or any other corneal insults that leave irregularity on the surface. A third group of patients I treat with complex corneas are those with higher-order aberrations or irregular astigmatism due to idiopathic or natural causes such as keratoconus.
The IC-8 IOL has also been found to enhance vision at all distances, with improved visual acuities and a broad range of continuous functional vision

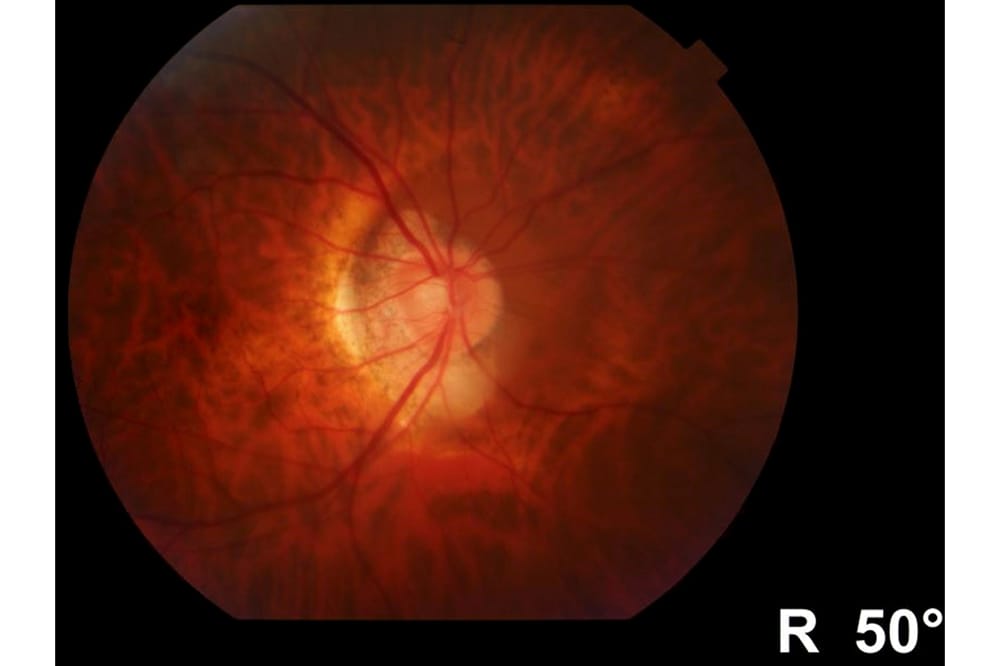
Fundal picture of optic disc through IC-8 implant.
Achieving consistent, reliable outcomes in these patients is difficult, and they are typically not candidates for traditional premium IOL technology. Multifocal technology can cause problems with glare and photopsia in patients with irregular astigmatism; therefore, traditionally we would implant bilateral standard monofocal lenses.1,2 Postoperatively, they will require glasses for intermediate and reading vision.
To get around the need for spectacles, we also have the option of monovision or blended vision, with one eye set for distance and one eye for either intermediate or near. This is a compromise, requiring adaptation, and patients can also lose a bit of stereopsis, which is of particular concern in elderly patients.
ENTER SMALL APERTURE TECHNOLOGY
The IC-8 IOL (AcuFocus), with its pinhole approach, provides the option of extending the depth of focus in one eye, allowing patients to gain intermediate and near vision. Even though we offset for a small amount of myopic correction, the IC-8 IOL provides good distance vision as well.

Visual field taken in patient with IC-8 implant.
As an aspheric monofocal lens with an embedded mask, the IC-8 IOL applies the small aperture principle to extend the depth of focus, providing an increased range of vision from far to near.3,4 The wavefront-filtering design eliminates unfocused peripheral light rays so that only the central rays focus on the retina.5 The small aperture design provides an extended depth of focus that makes the implant more tolerant of sphero-cylindrical residual refractive errors, compared with multifocal implants. The IC-8 IOL can tolerate up to 1.50D of corneal astigmatism.6
Studies have shown the IC-8 IOL can provide up to 3.00D of extended depth of focus and tolerate up to 1.00D deviation from the target manifest refraction spherical equivalent.7 This is in contrast to multifocal technology, where anything over 0.75D of residual sphere compromises visual acuity and spectacle independence, with the end result being unhappy patients.8 The IC-8 IOL has also been found to enhance vision at all distances, with improved visual acuities and a broad range of continuous functional vision.
IMPORTANCE OF IDENTIFYING COMPLEX CORNEAS
Cases of irregular corneas are often picked up incidentally – good tomography is key to a detailed examination in order to identify irregular astigmatism and higher-order aberrations. I prefer a Scheimpflug-based system to measure the irregularity and assess the aberrations in the cornea itself.
Although an obvious cataract is straightforward to identify, in patients with a dysfunctional lens and a smaller amount of opacity, it can be challenging to determine if the irregular astigmatism is coming from the cornea or the lens.
 Often I will supplement tomography with an aberrometry device that allows me to check the light scatter from the lens and the whole eye, and then differentiate each of those factors. In my practice, we use the KR-1W (Topcon) wavefront analyser and i-Trace (Tracey Technologies).
Often I will supplement tomography with an aberrometry device that allows me to check the light scatter from the lens and the whole eye, and then differentiate each of those factors. In my practice, we use the KR-1W (Topcon) wavefront analyser and i-Trace (Tracey Technologies).
THE SURGERY
The standard approach is to implant the IC-8 IOL monocularly. I check for eye dominance beforehand and place it in the non-dominant eye. In certain situations, such as idiopathic irregular astigmatism associated with keratoconus in an older patient, generally I will put the IC-8 IOL in the eye that has more severe cone and aberration. There are many benefits to having a small aperture in that eye.
The majority of my IC-8 IOL cases have been post-refractive surgery patients and I have obtained excellent outcomes. It is key to use very good, fourth-generation calculations such as Barrett True-K. Even then nothing is 100% accurate, so there is always a range. Typically with the IC-8 IOL, we are aiming for a little bit of under correction – anywhere from -0.50D to -0.75D. The landing zone with the IC-8 IOL is quite wide, so even with up to -1.00D, patients will obtain reasonable intermediate and near vision.

OCT RBFL taken in patients with IC-8 implant.
I use the femtosecond laser for creating the capsulorhexis in IC-8 IOL procedures. Because you’re looking through a small aperture, and certainly in cases where there may be a scar, laser centration is more accurate. Postoperatively, there have been studies that have shown no effect of the aperture on retinal visualisation both clinical and with optical coherence tomography (OCT), and on imaging devices for optic disc assessment.9
CONCLUSION
Current multifocal IOL technologies are typically contraindicated in patients with complex corneas stemming from a variety of causes including previous refractive surgery, keratoconus, and corneal scarring. This means these patients usually receive monofocal implants and are then left with a less-than-optimal range of vision that requires them to still rely on spectacles. Small aperture technology, leveraged by the IC-8 IOL on the other hand, can offer patients with corneal disease a premium outcome by overcoming associated visual disturbances to provide good functional vision for near, intermediate, and distance.
Jod S. Mehta, BSc (Hons.), MBBS, PhD, FRCOphth, FRCS (Ed), FAMS, is Distinguished Professor in Clinical Innovation in Ophthalmology and Head, Corneal and External Eye Disease Service, Senior Consultant Refractive Service at Singapore National Eye Centre. Prof Mehta is Executive Director, Head Tissue Engineering and Cell Therapy Group, Singapore Eye Research Institute; Deputy Vice Chair (Research) of Ophthalmology and Visual Sciences Academic Clinical Programme, SingHealth Duke-NUS Academic Medical Centre; Professor, Duke-NUS Graduate Medical School; Adjunct Professor, School of Material Science and Engineering, Nanyang Technological University; and Adjunct Professor, Yong Loo Lin School of Medicine, Department of Ophthalmology, National University of Singapore. He disclosed no financial relationships as related to the material discussed.
References
- Lee CY, Huang JY, Sun CC, et al. Correlation and predictability of ocular aberrations and the visual outcome after quadrifocal intraocular lens implantation: a retrospective longitudinal study. BMC Ophthalmol. 2019;19:188. https://doi.org/10.1186/s12886-019-1195-x.
- Woodward MA, et al. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009:35(6);992-997. DOI:10.1016/j. jcrs.2009.01.031: 19465282
- Grabner G, Ang RE, Vilupuru S. The small-aperture IC-8 intraocular lens: a new concept for added depth of focus in cataract patients. Am J Ophthalmol. 2015;160(6):1176- 1184. doi:10.1016/j. ajo.2015.08.017.
- Dick HB, Piovella M, Vukich J, et al. Prospective multicenter trial of a small-aperture intraocular lens in cataract surgery. J Cataract Refract Surg. 2017;43(7):956- 968. doi:10.1016/j.jcrs.2017.04.038.
- Tucker J, Charman WN. The depth-of-focus of the human eye for Snellen letters. Am J Optom Physiol Opt. 1975;52(1):3-21. doi:10.1097/00006324-197501000-00002.
- RE Ang. Small-aperture intraocular lens tolerance to induced astigmatism. Clin Ophthalmol 2018;12:1659-1664.
- Ang RE. Visual performance of a small-aperture intraocular lens: first comparison of results after contralateral and bilateral implantation. J Refract Surg. 2020;36(1):12-19. doi: 10.3928/1081597X-20191114-01.
- Braga-Mele R, Chang D, Dewey S, et al. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014;40(2):313–322
- Srinivasan S, Khoo LW, Koshy Z. Posterior segment visualization in eyes with small-aperture intraocular lens. J Ref Surg. 2019;35:538-542. https://doi.org/10.3928/10815 97X-20190710-01.





