
Looking after patients with cataract is likely to be a common part of your day-to-day clinical practice. However, cataract surgery is an ever-evolving procedure, with constant advancements in intraocular lens (IOL) technology. Patients are becoming more knowledgeable and demanding, especially regarding unaided visual quality. The following review will discuss new and emerging technology that will be available to your patients.
NEW ZEISS INTRAOCULAR LENS
 In my experience, in both the private and public hospital systems, the most popular monofocal IOL in Australia at present is the Johnson and Johnson Tecnis IOL. The Alcon Clareon is also a very popular IOL. Both IOLs are made from a hydrophobic acrylic material, which is the most used material group, due to a number of positive properties. Firstly, they are amenable to the generally preferred single-piece C-loop haptic design, as the materials have a very low water content, a high refractive index, and usually, a high memory. This group of materials unfolds in a controlled fashion, and most surgeons find the implantation process safe and reliable (Figure 1).
In my experience, in both the private and public hospital systems, the most popular monofocal IOL in Australia at present is the Johnson and Johnson Tecnis IOL. The Alcon Clareon is also a very popular IOL. Both IOLs are made from a hydrophobic acrylic material, which is the most used material group, due to a number of positive properties. Firstly, they are amenable to the generally preferred single-piece C-loop haptic design, as the materials have a very low water content, a high refractive index, and usually, a high memory. This group of materials unfolds in a controlled fashion, and most surgeons find the implantation process safe and reliable (Figure 1).
Traditionally, the Zeiss portfolio of IOLs is made from a hydrophilic acrylic material, with a four-point haptic design. Hydrophilic acrylic IOLs have a high-water content. Hydrophilic acrylic is probably the most uveal biocompatible of all IOL materials, which may be an important consideration for cataract surgery in eyes with chronic uveitis, for example.
One major problem with some hydrophilic acrylic lenses is opacification of the optic material due to calcification. This can occur spontaneously, or after subsequent corneal or vitreo-retinal surgery.1 Some cases have needed subsequent explantation due to poor optical quality.
HYPOTHETICAL SCENARIO
OD: -1.50 / -0.75 x 90 → 6/12, N6 unaided,
OS: -2.00 DS → 6/9, N5 unaided.
Clinically, you found significant progression of his cataracts, with a small myopic shift. The rest of his ocular examination was unremarkable. Mr Schmidt has done some research on cataract surgery and would like your opinion.
As a mechanical engineer, Mr Schmidt is meticulous and appreciates precision. He is an amateur photographer and rates Zeiss camera lenses as giving the best image quality. He would like your opinion on the new Zeiss CT Lucia IOL.
What advice would you give him regarding the CT Lucia and cataract surgery in general?

Figure 1. Tecnis (left) and Clareon (right) IOLs.
Zeiss CT Lucia
Zeiss has recently brought a new IOL to market, the CT Lucia 621P/PY. The non-toric version is already available in New Zealand and will be available in Australia this month (November 2022). The toric version will be coming, though the timeline is not definite.
Similar to market leaders Tecnis and Clareon, the Zeiss CT Lucia is a hydrophobic acrylic aspheric monofocal IOL. It is a single-piece IOL with step-vaulted haptics and a 6.0mm optic that has a sharp posterior edge and an innovative aspheric design, which as described below, is an interesting feature.
The CT Lucia is available in versions with or without blue light filtering, 612P and 621PY respectfully (Figure 2). Compared with hydrophilic acrylic IOLs, hydrophobic acrylic IOLs are associated with less posterior capsular opacification (PCO).2 The development of PCO is further limited by the sharp posterior edge of the CT Lucia.
The CT Lucia comes preloaded in a single-use injector system, which is the preferred method to allow for an easy and safe cataract surgery workflow. Unfolding in the capsular bag is facilitated by its heparin-coated surface.3
One major problem with some hydrophilic acrylic lenses is opacification of the optic material due to calcification. This can occur spontaneously, or after subsequent corneal or vitreo-retinal surgery

Figure 2. Zeiss CT Lucia 612PY (left) and 621P (right).
Spherical Aberration
Spherical aberration in the human eye is a combination of the positive spherical aberration of the cornea, and the negative spherical aberration of the crystalline lens. In young eyes, the positive spherical aberration of the cornea is compensated by the negative spherical aberration of the lens; as a result, overall spherical aberration in the young eye is low. As the eye ages, the optical properties of the crystalline lens change, resulting in overall positive spherical aberration and decreased optical performance. Spherical aberrations generally reduce the contrast of the retinal image and affect visual performance, especially under mesopic conditions.4
Conventional spherical IOLs add approximately 0.08μm (over a 4mm pupil) positive spherical aberration to the preexisting aberrations caused by the cornea, increasing the total spherical aberration of the eye. In 2002, an aspheric IOL design was introduced to compensate for the positive spherical aberration of the cornea. Aspheric IOLs generate negative spherical aberration, leading to a smaller amount of post-operative spherical aberration as compared to spherical IOLs. These IOLs are said to be spherical aberration correcting.
Currently, the vast majority of IOLs used in Australia are aspheric, as studies consistently show that post-operative contrast sensitivity is significantly better with aspheric IOLs when compared to spherical IOLs. However, with IOL decentration, optical quality with aspherical IOLs deteriorates due to coma.
The aspheric Zeiss CT Lucia is designed such that the IOL is aberration correcting in the central zone but becomes aberration neutral in the periphery. This design preserves the contrast sensitivity across a range of potential decentrations and ensures best visual function, even in low lighting conditions. So, the CT Lucia has the advantages of an aberration correcting IOL while minimising the risk of coma with decentration. Risk factors for IOL decentration include pseudoexfoliation and zonular insufficiency due to trauma.
PREVIOUS LASER REFRACTIVE SURGERY
Modern cataract surgery is considered a refractive procedure. With advances in biometry, IOL prediction formulas, IOL technology and surgical refinement, most cases now fall within +/- 0.5 dioptres of prediction post-operatively. However, there are cases where the predicted refractive outcome is not achieved. This is particularly true in eyes that have previously had laser refractive surgery, such as our patient, Mr Schmidt. This is due to issues with the calculation of the IOL power.
Figure 3. Rayner Sulcoflex (left) and the Medicontur 1stQ AddOn (right).
Since 1975, IOL power has been predicted, or calculated, using measurements of the corneal power and axial length. The most successful early IOL calculation formula was the SRK formula:
P = A – 2.5L – 0.9K
Where P = IOL Power, A = a constant number corresponding to a particular IOL, L = axial length, K = average keratometry (K1 + K2)/2.
Over the years, more accurate formulas have been developed, incorporating more data, such as the anterior chamber depth, corneal diameter, and lens thickness. Improved predictability has also been gained by technological advancements, allowing more accurate measurement of this data. In essence, all IOL calculation formulae are trying to predict where the new IOL will sit in the eye (the effective lens position), and therefore the power that the IOL should be to achieve a desired refractive outcome, based on the anatomy of the eye.
In eyes that have had previous laser refractive surgery, there are two main issues that lead to IOL power prediction errors. Firstly, current keratometers do not correctly measure central corneal power in these eyes, because they instead measure the curvature of the anterior corneal surface. This measurement is converted into keratometric diopters, with a standardised keratometric index of refraction (usually 1.3375). The keratometric index of refraction refers to a theoretical single refractive lens, representing the anterior and posterior corneal surfaces, and assumes a stable ratio of anterior-to-posterior corneal curvature. Of course, LASIK and PRK disrupt this ratio, making the standard keratometric index of refraction invalid.
The second problem is that by using these inaccurate K-values, the formula will incorrectly predict the effective lens position. Both errors lead to an underestimation of the required IOL power in eyes that had previous myopic refractive surgery, and an overestimation of the required IOL power in eyes that had previous hyperopic refractive surgery. As such, patients who require cataract surgery after LASIK or PRK should be informed that they may require a second procedure to achieve their desired refractive target.
Piggyback Intraocular Lenses
To correct residual refractive errors after routine cataract surgery, a second IOL can subsequently be inserted into the eye. This is a relatively easy and atraumatic procedure that is not associated with the risk of potential complications seen with IOL exchange or performing corneal refractive surgery on an eye that has already had LASIK in the past.
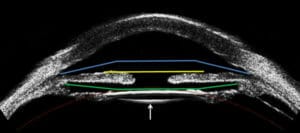
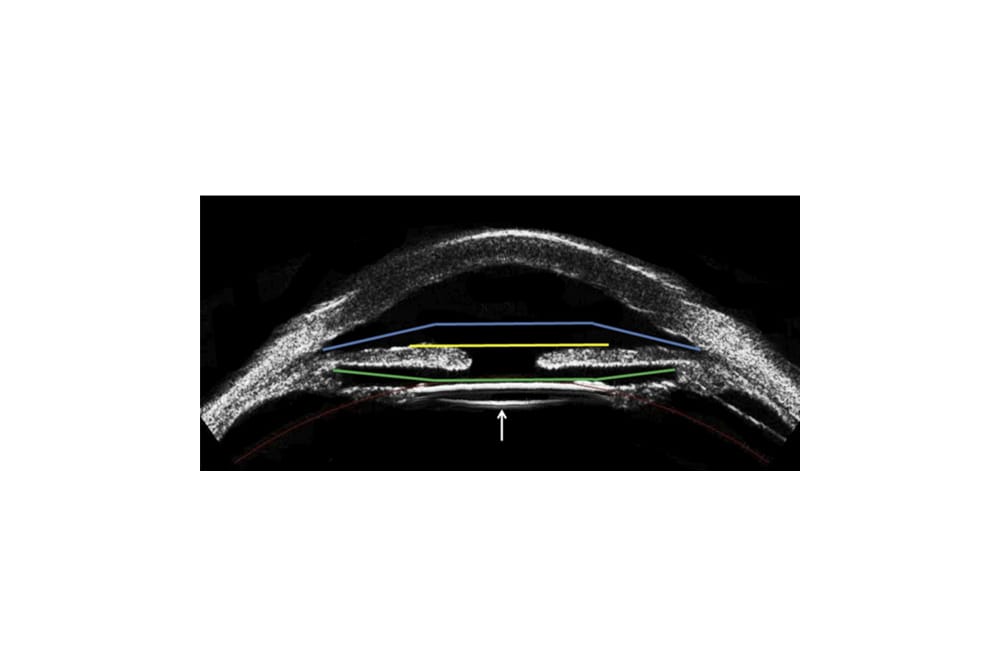
Figure 4. High-frequency ultrasound of the anterior segment of a human eye containing an IOL located in the capsular bag (arrow). The coloured lines indicate the other sites where an IOL can be fixated. The green line indicates the ciliary sulcus.
In Australia, the two most common piggyback IOLs used are the Rayner Sulcoflex and the Medicontur 1stQ AddOn (Figure 3). These lOLs sit in the ciliary sulcus, behind the pupil, and in front of the original posterior chamber IOL in the capsular bag (Figures 4 and 5). Patients who have loose zonules from trauma, or pseudoexfoliation, are not good candidates for piggyback IOLs. The calculation for the lens power is based on subjective refraction.
The Sulcoflex IOL is made from a hydrophilic acrylic material and has special design features to reduce complications that might develop from sulcus placement. The IOL has large, 14mm undulating round-edged haptics, with a 10-degree angulation that reduces the risk of contact with the posterior iris pigmented epithelium and subsequent pigment dispersion. The IOL has a roundedged 6.5mm optic to prevent optic-iris capture and reduce the likelihood of edge glare and dysphotopsias.
The Sulcoflex IOLs come in aspheric monofocal, toric, and multifocal versions. The multifocal is a refractive bifocal IOL with a +3.5D add that yields a +3D add at the spectacle plane. The availability of a piggyback multifocal IOL opens this refractive option to patients who did not have a multifocal IOL with their primary cataract surgery. In addition, sulcus placement allows for easy removal if patients are unhappy with any optical aberrations from the multifocal optics. The explantation of a Sulcoflex IOL is much safer and easier than a standard posterior chamber IOL in the capsular bag.
The 1stQ AddOn IOL is also made from a hydrophilic acrylic material with a 6mm optic diameter and an overall diameter of 13mm. It has four soft flexible haptics, a convexconcave optic, and a square shape to improve stability in the sulcus, reduce edge light scatter and help maintain a constant distance between it and the posterior primary lens. The toric model has the cylinder correction on the front surface. Other combinations of lens on this platform include a trifocal, a trifocal toric, and the Scharioth Macula Lens (SML). This latter IOL has a high-powered central addition for macular degeneration patients. The AddOn trifocal and trifocal toric lenses are provided with addition powers of +3.0 and +1.5D in the sulcus plane (near reading adds of 37.5cms and 74cms).
Figure 5. Slit-lamp cross-sectional view of a piggyback IOL.
With the addition of the 1stQ Addon trifocal IOL a ‘dual lens’ procedure is possible. This procedure involves the implantation of two IOLs during the same surgery, with the aim being multifocal correction. Initially a monofocal or monofocal toric IOL is placed into the capsular bag. Immediately thereafter, a plano powered trifocal 1stQ AddOn IOL is placed above the original lens into the sulcus. The dual procedure offers a safe and reversible solution for patients who are unsure about receiving multifocal in-the-bag implants. Moreover, the ability to reverse the procedure can be very useful in situations where patients are prone to develop ocular disease later in life, such as macular degeneration, in which case removal of the multifocal component may be advantageous to the patient to maximise contrast sensitivity.5
Light Adjustable Intraocular Lenses
Currently available in the United States of America, the RxSight Light Adjustable Lens (LAL; Figure 6) may be the most predictable way to provide optimal visual outcomes for cataract surgery patients like Mr Schmidt who have previously had laser refractive surgery.
The LAL can be precisely optimised after its implantation if the desired refractive result is not achieved. The LAL is made from a photo-reactive UV-absorbing silicone, not acrylic, material. It incorporates proprietary silicone photoreactive additives called macromers, which are distributed throughout the lens. When light is directed to a specific area of the lens, macromers in the path of the light attach to the ends of other macromers, forming polymers. The remaining unreacted macromers physically diffuse into the exposed area, causing a highly predictable change in the curvature of the lens. As long as there are unpolymerised macromers, further adjustments to refine the refractive power can be made by applying light to different areas of the lens.
The LAL has a standard three-piece design with a 6mm optic diameter and a 13mm overall length. After a period of post-operative refractive stabilisation (approximately two weeks after surgery), the lens is adjusted noninvasively. Postoperative adjustments can range from -2 to +2D sphere and from 0.5 to 3D cylinder in any combination.
Up to three office-based adjustments, each taking approximately 90 seconds, can be made to fine-tune refractive outcomes. The office-based Light Delivery Device (LDD) resembles a slit-lamp Nd:YAG laser. Once the patient’s vision is optimal, the IOL is permanently ‘locked in’ at its current refractive state, preventing further power changes. The LAL is sensitive to UV-A light until the adjustment process is completed, so until final lock-in, patients must wear UVprotective glasses to avoid incidental exposure from sunlight. This inconvenience may prevent the LAL from being used widely in routine eyes.
Results with the LAL in post-refractive surgery eyes have been published. In Brierley’s retrospective study of 34 postrefractive surgery eyes in 21 patients, the mean refractive spherical equivalent, relative to target refraction after final lock-in with the LAL, was within +/-0.25D in 74% of eyes, +/-0.50D in 97% of eyes, and +/-1.00D in 100% of eyes.6 These results were 60% more predictable than the best refractive outcomes achieved in previous studies, with monofocal IOLs in post-refractive surgery eyes.7
IOL Power Adjustment by Femtosecond Laser
The ability to change the power of any IOL in a non-invasive manner at any time post-operatively would be revolutionary. The obvious clinical relevance would be in challenging refractive cases, such as in postrefractive surgery eyes like Mr Schmidt’s. However, the use would extend to even routine eyes post-cataract surgery who may develop a refractive error years after their primary cataract operation.

Figure 6. RxSight Light Adjustable Lens.
Experimental work by Sahler8 has shown that it is possible to create a negative refractive index change in a hydrophobic acrylic material by exposing the material to water and low energy light from a femtosecond laser at 520nm wavelength. Application of the laser induces chemical reactions within targeted areas in the substance of the IOL optic, under the surface of the optic. This approach, known as refractive index shaping, is an exciting new technology being developed by Perfect Lens. One of the most interesting aspects of this technology is that it can be applied to any commercially available hydrophobic or hydrophilic acrylic IOL, so a special IOL material is not necessary.9
In vitro and ex vivo studies have demonstrated the accuracy and repeatability of refractive index shaping and have shown that the optical quality of the lens is not significantly affected by multiple treatments. Femtosecond laser technology can even be used to create multifocality in a monofocal lens, and it can also cancel a diffractive multifocal add on a traditional multifocal IOL. Creation of a toric change of up to 7.60D in a monofocal hydrophobic acrylic lens has been demonstrated. An initial in vivo (rabbit) study has been successfully completed.10
This approach to postoperative power adjustment has potential advantages over other IOL power-adjustable technologies because it could be applied to many commercially available acrylic IOLs. Additionally, it would not depend on a special IOL material, and there would be no time restrictions regarding when it can be done post-operatively. The ability to customise spherocylindrical treatment, and to place or remove multifocality, would create a paradigm shift in how we address our patient’s IOL choices.10
HYPOTHETICAL SCENARIO REVISITED
Mr Schmidt’s previous myopic LASIK would have increased the amount of spherical aberration in his cornea. As such, an aspheric IOL that can correct some of this spherical aberration would be preferred to a spherical IOL. The Zeiss CT Lucia is an aspheric IOL, and hence would be an appropriate choice.
Mr Schmidt, like all patients undergoing cataract surgery, should be informed that multifocal IOLs, or monofocal IOLs with a monovision arrangement, are possible. However, his personality will likely contraindicate these options. Low myopes are accustomed to good unaided reading vision, and hence Mr Schmidt may feel that his near vision with multifocal IOLs or monovision is worse than pre-operatively. A refractive aim of -1.5 to -2Ds bilaterally may be the best option for him.
In the future, the Light Adjustable Lens may be available in Australia. However, this would require the use of a silicone IOL, and Mr Schmidt would have to wear UV-protective glasses until the power of the IOL is locked-in. Alternatively, if Mr Schmidt had the Zeiss CT Lucia implanted, as is his wish, there may become technology available in the future to refine the power of the IOL using a femtosecond laser.
To earn your CPD hours from this article visit mieducation.com/cataract-surgery-new-andemerging- technology.
Dr Jay Yohendran is a Sydney-based ophthalmologist who specialises in refractive cataract surgery. He is a member of the Royal Australian and New Zealand College of Ophthalmologists, as well as the Australasian Society of Cataract and Refractive Surgeons. He is locally trained and completed the Graduate Diploma of Cataract and Refractive Surgery at Sydney University. Dr Yohendran is the Founder and Medical Director of Northern Sydney Cataract on Sydney’s lower North Shore, and he performs cataract surgery at Chatswood Private Hospital. He is the Head of the Ophthalmology Department at Royal Prince Alfred Hospital and a Clinical Lecturer at Sydney University.
References
- Morgan-Warren PJ, Andreatta W, Patel AK. Opacification of hydrophilic intraocular lenses after Descemet stripping automated endothelial keratoplasty. Clin Ophthalmol. 2015;9:277–283.
- Ying Li, Jiaxing Wang, Zhuo Chen, Xin Tang. Effect of hydrophobic acrylic versus hydrophilic acrylic intraocular lens on posterior capsule opacification: meta-analysis. PLoS One. 2013:8(11):e77864.
- Schmid R. Early experience with the aspheric CT Lucia 621P IOL. Host of design features add up to reliable optical performance. Ophthalmology Times Europe. Oct 2020.
- Majid Moshirfar, MD. Spherical Aberration of Intraocular Lenses. J Ophthalmic Vis Res. 2010;5(4): 215–216.
- Apel A, Harrisberg B. 1stQ Secondary Sulcus Supplementary IOLs: Innovative Applications For Multifocal Correction. mivision education.
- Brierley L. Refractive results after implantation of a light-adjustable intraocular lens in post-refractive surgery cataract patients. Ophthalmology. 2013;120:1968-1972.
- Hengerer F. Use of the Light Adjustable Lens after Corneal Refractive Surgery. CRST Europe. June 2017.
- Sahler R, Bille J, Sean E, Chhoeung S, Chan K. Creation of a refractive lens within an existing intraocular lens using a femtosecond laser. J Cataract Refract Surg. 2016;42(8):1207-1215.
- Werner L, Mamalis N. IOL Power Adjustment by Femtosecond Laser. CRST Europe. June 2019.
- Tran D. Perfect Lens. CRST. May 2018.





