

Glaucoma specialists gathered in Hobart, Tasmania in late February to share their knowledge and experiences on diverse glaucoma-related topics at the Australian and New Zealand Glaucoma Society Congress 2024 (ANZGS 2024). Here we review some of the lectures presented over three days on Australia’s Apple Isle.
The prestigious Lowe lecture was presented by Professor Linda M. Zangwill from the University of California in San Diego, who spoke on ‘Harnessing artificial intelligence to improve glaucoma management: Opportunities and challenges’.
Prof Zangwill said ophthalmology was leading the way in its practical application of artificial intelligence (AI), which she said could be described as “the fourth industrial revolution”.
“As everyone knows, artificial intelligence is really changing our lives… ophthalmology is really key to this whole process in transforming healthcare. Generative AI is disrupting lives… it’s really quite amazing and it’s transforming healthcare.”
She said one of the reasons ophthalmology was leading the way in AI was the large datasets available with “good quality ground truth” such as retinal photographs, optical coherence tomography, patient records, ophthalmology registry data, and public data sets.
AI-based tools had the “potential to improve the accuracy and consistency of glaucoma management”, she said.
“If you have a couple of glaucoma specialists look at a photo, well, how often do they agree? But we can really automate the glaucoma detection for underserved areas, telehealth, as well as in your clinic,” Prof Zangwill told the conference audience.
AI had the potential to provide clinical decision support as well as analytics that could lead to a higher level of personalisation in medicine, by predicting “who is at the highest risk of progressing, who might need surgery in the future”.
“So, we can really move from a one size fits all to personalised glaucoma management. Instead of having visual fields every six months, perhaps we’ll have the right diagnosis, the right test, and the right frequency for that individual patient.”
Prof Zangwill talked about the ways to improve AI and machine learning but said the key would be data management.
“People say that 90% of AI is data management. Where’s your ground truth coming from? How are you bringing all this to where the computer is? So, I just want to share that as one of the challenges.”
She said other challenges included bias and how the results were integrated in clinical settings. “And then there’s… regulatory privacy, medical malpractice, et cetera. But there’s tremendous opportunities for detection of glaucoma, prediction of disease, clinical decision support, and new insights into glaucoma pathophysiology.”
TAKING A GRAFT CHANCE
The Gillies lecture was presented by Professor Graham Lee, University of Queensland, Brisbane, who drew on his interest in cornea and glaucoma to speak about corneal endothelial disease and glaucoma; glaucoma surgery causing endothelial decompensation; and post keratoplasty glaucoma.
Among several case studies, Prof Lee reported on a patient he recently saw with severe keratitis that had occurred within just two days. He had no history of trauma, herpes simplex or diabetes. The patient had light perception only in this eye, however the B scan showed no endophthalmitis. His other eye was healthy. Although it was suggested that he perform a primary enucleation, Prof Lee decided that with a clear B scan, “you’ve got to do something” and so he chose to do a large corneoscleral graft.
“We started at 10 o’clock at night … we finished about 2am,” he said. Prof Lee said for these procedures, the key is to maintain limbal stem cells and the trabecular meshwork, “otherwise you’re going to lose the eye anyway (from stem cell failure and glaucoma)”.
After performing a lamellar limbal dissection while removing infected tissues (Figure 1), he said “when you cut the cornea, you have to use your scissors horizontal to the floor to preserve the Schlemm’s canal as much as possible. The stitching takes a lot of time – the principle is you just keep stitching until it stops leaking and just keep hoping and praying there is no expulsive haemorrhage.” Prof Lee reported that at 10 weeks the ocular surface was healed with an intraocular pressure of six. “The patient did all right… he was a happy camper”.
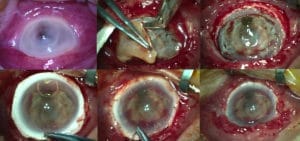
Figure 1
A LION’S SHARE OF OCULAR PATHOLOGY
A number of interesting cases were presented to the audience, with invitations for discussion on treatment options.
In a presentation replete with groan-worthy ‘Dad jokes’, Dr Hamish Dunn presented on the case of a 26-year-old lion keeper with a complex history.
“She had congenital cataract, she’s now a phakic, she’s got an axial length of 29. She’s had recurrent retinal detachments. She doesn’t have silicone oil in currently, but there’s a bit of emulsified oil in the angle and she’s got a risk of another detachment down the track.
“She’s had cystoid macular oedema that’s now settling and she’s a steroid responder.”
The woman wanted to have a baby, and much of the presentation centred on the suitability of various treatments for women who are pregnant or breastfeeding.
The case prompted lively discussion, with Dr Dunn revealing that he “put a pars plana tube in, which has worked remarkably, and we’ve kept the supramid suture in and so the oil’s not currently migrating, and she’s got a pressure of 15, five months down the track”.
ITRACK DATA ON CANALOPLASTY
Dr Nathan Kerr, from the Centre for Eye Research Australia, delivered a presentation outlining the 24-month results of the iTrack Global Data Registry to support the role of canaloplasty for treatment of glaucoma.
His co-authors were Dr David Lubeck, Assistant Clinical Professor of Ophthalmology at the University of Illinois in the United States, who also presented to the conference, and Dr Keith Barton, from Moorfields Eye Hospital in the United Kingdom.
Dr Kerr said there was “renewed interest in canaloplasty” as a minimally invasive procedure that was implant free, “and so that can appeal to some patients”.
“It certainly minimises the risk of any endothelial cell loss from an implant, but I’d like to advocate it can also be combined with a stent procedure should that be clinically indicated. To me, the real benefit is its comprehensive nature,” Dr Kerr said.
He said preliminary 24-months results came from data from 20 sites across the United States, Canada, Europe, Asia, and Australia.
“We have 395 eyes to date. The majority have mild or moderate disease, but we also see that… surgeons are using this in patients who have advanced and severe disease.
“Most, of course, were on-label indications of primary open angle glaucoma. But, being a real-world Registry, we also collect off-label indications…”
Dr Kerr said most cases were performed in combination with cataract surgery, with only about one in 10 performed as a standalone procedure.
“And so, what we can see is for the vast majority of eyes, they’re achieving lower pressures.”
He said medication use also changed postoperatively, going from a mean of two to “the vast majority of patients being medication free”.
Dr Kerr said the data revealed postoperative complications were very rare, with “all resolved without any intervention… and to date, no eyes have required a further glaucoma procedure”.
“And we saw an exceptionally good safety profile; 99.2% didn’t have any intraoperative complication. And from 395 eyes, there was only one case of a Descemet’s membrane detachment.
“This study helps give further weight to the role of canaloplasty, another tool in our armamentarium for these patients achieving approximately 30% reduction in IOP and approximately 50% reduction in medication burden after surgery.
“We saw these benefits across both standalone and combined cases through varying types and stages of glaucoma,” Dr Kerr told the conference audience.
Following Dr Kerr’s presentation, Dr Lubeck described the multicentre canaloplasty data registry as “probably the cleanest set of realworld large data sets on glaucoma that could possibly be put into AI models as a starting point to get the most reliable data going forward”.
With large data sets built with diverse patient inputs, he said “we are bridging human intelligence and AI now, to hopefully come to more relevant conclusions about clinical efficacy”.
The knowledge gained from the canaloplasty data registry may inform clinical decisions on the type and volume of ophthalmic viscosurgical devices (OVD) used in relation to glaucoma type, stage and severity, and the level of intraocular pressure. Additionally, it may help predict IOP and any decrease in medication required post-canaloplasty.
SLEEP APNOEA SYNDROME
Dr Ella Berry MChD, a second-year ophthalmology trainee, spoke on a study she conducted with colleagues from the Flinders Centre for Ophthalmology, Eye and Vision Research, on sleep apnoea syndrome and its correlation with progression of normal tension glaucoma (NTG).
Sleep apnoea syndrome is a sleep disorder characterised by repeated periods of upper airway obstructions leading to fluctuations in blood oxygen and carbon dioxide levels. This disorder affects approximately one billion people globally, many of whom remain undiagnosed.
Building on the hypothesis that transient low oxygen and increased vascular resistance due to sleep apnoea compromises optic nerve head perfusion and contributes to the progression of NTG, Dr Berry conducted a study with 325 participants from the PROGRESSA1 study to investigate the association between sleep apnoea syndrome and longitudinal structural and functional changes in a cohort of normal tension suspects and early manifest glaucomas.
Participants from the PROGRESSA study wore a wrist-worn peripheral pulse oximeter that measured blood oxygen levels every four seconds for three consecutive nights to determine their oxygen desaturation index (ODI). Using oximetry data to determine a patient’s sleep apnoea status, this status was correlated with their rate of macular ganglion cell-inner plexiform layer (mGCIPL) thinning and rate of visual field change.
The findings from this study revealed that, among the normal tension cohort (159 participants), individuals diagnosed with sleep apnoea (27 participants) exhibited faster rates of mGCIPL thinning and more rapid visual field deterioration than those participants without sleep apnea. Additionally, the study highlighted that the severity of oxygen desaturation was correlated with the pace of the mGCIPL thinning.
Dr Berry’s recent research found a correlation between lower body mass index (BMI) and glaucoma disease progression in three large cohorts.2 Similarly, in this current study, a lower BMI was associated with both a faster rate of mGCIPL thinning and a faster rate of visual field deterioration. Dr Berry emphasised the importance of recognizing that participants exhibiting these patterns were not necessarily overweight. Healthcare providers should still consider investigating sleep apnoea in nonoverweight patients with glaucoma progression.
“Assessing for nocturnal hypoxemia with sleep apnoea testing is an easily modifiable factor that can be addressed by both patients and clinicians to assist with the NTG risk profiling,” she said.
PORTABLE PERIMETRY TESTING
Dr Neira John, now a glaucoma Fellow at the Royal Victorian Eye Ear Hospital, spoke about a project she worked on as a Registrar in 2023, looking at portable perimetry within the emergency department at Sydney Eye Hospital.
Noting that Humphrey visual field analysers are the gold standard for perimetry in diagnosing and monitoring glaucoma, she said drawbacks include expense, the need for trained operators to supervise patients during testing, and the device’s lack of portability.
Her project involved trialling three portable perimeter analysers developed with the aim of overcoming these drawbacks (Melbourne Rapid Fields, the Eyeonic, and Olleyes, which uses a virtual reality headset). Each device was comparable with Humphrey visual field analyser testing, was well-supported, and approved by the Therapeutic Goods Administration. Without being comparative or scientific, the aim of the study was to assess efficiency, integration with the emergency department’s workflow, and user experience.
Each device was trialled over 30 days, with patients and clinicians interviewed about their experiences, and a focus group discussion at the end of the trial.
Thirty-six patients were recruited – 23 for each device – with a mean age of 44 years. Just under half were female and they had presented at the emergency department with conditions such as headache, optic nerve disorders, and stroke. Just over half had experienced perimetry testing before.
Dr John described the features and user protocol for each device. She reported that broadly, the patients were happy with all of them: half preferred portable perimetry, a third had no preference, and 20% preferred standard perimetry. Patients acknowledged the clarity of instruction with the portable devices.
Clinicians were also broadly happy with all of the devices, finding them very easy to use and time efficient.
Focus group discussions determined that portability was a preferred feature, as was cloudbased data storage, and the ease of making PDFs, which could then go electronically into patients’ records or be printed out.
The orthoptists particularly liked using Olleyes with patients who were bedbound, or wheelchair bound due to ease of use and positional comfort (for both patient and clinician).
Different language options on Melbourne Rapid Fields and Olleyes were appreciated. They noted that all three devices caused a feeling of disorientation for some patients.
Dr John concluded by saying that based on the relative strengths of each device, Sydney Eye Hospital had applied to use all three.
REDEFINING COLLABORATIVE CARE
Dr Anne Lee spoke about the work of RANZCO’s Collaborative Care in Glaucoma Working Group to redefine an effective model of care for people living with glaucoma. She said that with an ageing population, by 2070 there will be approximately one million people in Australia living with this chronic disease which “requires ongoing surveillance” and “consumes a lot of resources”.
Dr Lee is a member of the RANZCO’s Vision 2030 working group charged with redesigning a collaborative model for glaucoma care that overcomes current barriers to address inequalities and increase access to healthcare, while minimising duplication of efforts and reducing the burden of glaucoma management and treatment.
She described the definition of collaborative care as “contentious”, and not strictly limited to optometry.
Collaborative care is “an integrated approach where two or more providers are involved with and communicate with a patient’s diagnosis”. In the past 10 years, several models of collaborative glaucoma care have been established. Dr Lee said the models vary across different regions, and can involve ophthalmologists, orthoptists, optometrists, nurses, and general practitioners, depending on whether they are being delivered via public vs private hospitals, optometry practices, private ophthalmic practices, university settings, Aboriginal health services or in general practice. Models also differ according to whether the patient has a coexisting disease and whether they are being seen in person, via telehealth et cetera.
There are three phases in the collaborative care project and the working group is at phase one, which is “to assess and evaluate what is out there at the moment and possibly to develop novel approaches, refine the eligibility criteria for collaborative programs, identify the challenges that may be ahead and how we can overcome them, and define the role of our co-collaborators – all with stakeholder consultation.”
Phase two is to provide a non-prescriptive report and recommendation that will assist people who want to go into various models. Phase three is monitoring and implementation.
The Department of Health has received a pre-budget submission requesting more support to develop ongoing collaboration care models between eye care stakeholders.
The working group is planning a workshop in Sydney mid this year, which will enable interested healthcare providers and advocates to provide constructive feedback on future models of collaborative care.
In 2025, the ANZGS Congress will be held in Perth, Western Australia.
References
- FFitzgerald, J., Usher, B., Craig, J., et al., Baseline data of patients enrolled in PROGRESSA study: glaucoma suspect and early manifest glaucoma progression trial. Clinical and Experimental Ophthalmology. 2013 Nov;41:81–81.
- Marshal, H., Berry, E.C., Torres, S.D., et al., Association between body mass index and primary open angle glaucoma in three cohorts. American Journal of Ophthalmology. 2023 Jan;245:126–133.






