While there is still much to learn – and evidence to be gathered – about the impact of lifestyle and diet on dry eye disease, research by the Tear Film and Ocular Surface Society (TFOS) is now shining the light on the guidance eye care professionals can provide to help patients struggling with this debilitating condition.
Dry eye can have a significant effect on a person’s lifestyle and can be a challenging condition to treat as practitioners. Often it seems that mainstay treatments fail to be effective, and the reason why seems unclear. In April 2023, TFOS published results from the A LifeStyle Epidemic: Ocular Surface Disease workshop.1
Eight reports looked at evidence-based literature on how cosmetics, contact lenses, digital eye strain, elective medications and procedures, climate, lifestyle, nutrition, and societal challenges impact the ocular surface. While many findings are not yet able to be supported with high-quality evidence, they open the door to further research on how specific factors
affect the eye surface. Additionally, the findings begin to lift the confusion on our recalcitrant dry eye cases, highlighting the importance of looking at our patients holistically for best treatment and management.
This article takes a deep dive into the presentations of two patients to explore further the impact of lifestyle on dry eye.
Patient One
Irene Jacob* is a woman in her mid-60s, who presented with a six-month history of gritty, dry, and sore eyes. She recalled having similar symptoms 30 years prior when she was diagnosed with Graves’ disease. At that time, she had radioactive iodine treatment, but eventually required oral thyroxine replacement for an underactive thyroid, managing any subsequent ocular irritation effectively with artificial tears. Twenty years ago, she underwent bilateral laser-assisted in situ keratomileusis (LASIK) surgery (repeated a month later) with no reported dry eye symptoms at the time. Her only other medication was Simvastatin for her cholesterol and a hormone replacement therapy (HRT) gel following a hysterectomy in her early 40s. An updated refraction did not help her symptoms, and her optometrist diagnosed dry eye disease (DED). Initially, the cause of her most recent symptoms were not apparent. Obvious risk factors of refractive surgery, thyroid, and HRT were decades earlier and appeared to have no relation to her current presentation.
To treat DED well, it is important to work out why the patient has it, as well as the triggers. Ms Jacob couldn’t recall anything changing in the prior six to 12 months that could explain the exacerbation of her symptoms. I explained the recent Lifestyle workshop findings and started by questioning if she had any ‘inflammatory’ conditions – even something like an old injury that gave her pain. She had broken her pelvis in an accident three years prior, and over the past 12 months it had become very painful, resulting in her sleeping poorly. Of even more interest, her personal life had become overtly stressful in the past six months and she had periods of depression. It began to be quite clear to me that her recent lifestyle events were the triggers for her once again symptomatic DED. As we continued her history, it turned out that she also had a long history of irritable bowel syndrome (IBS) and had been on a low FODMAP diet (fermentable oligosaccharides, disaccharides, monosaccharides) for the past six years to control it.
Patient Two
Mary Bliht* is a woman in her mid-40s who was diagnosed with Sjögren’s syndrome 15 years ago, and usually managed her ocular surface symptoms well with non-preserved gel and artificial tears. She was diagnosed with breast cancer and underwent chemotherapy treatment from October 2022 to February 2023 (she noted her dry skin and mouth were exacerbated by the treatment) with subsequent surgery. Ms Bliht’s medications included hydroxychloroquine and tamoxifen and she had a long history of using selective serotonin reuptake inhibitors (SSRI). After an episode of conjunctivitis following an international holiday in 2023, her dry eye symptoms suddenly became unmanageable, causing increased glare sensitivity and blur.
She also reported being a poor sleeper and a long history of IBS.
Ms Jacob and Ms Bliht presented to my practice in early 2024. Both worked in air- conditioned environments and their jobs were screen based.
Discussion
The goal of the TFOS Lifestyle Workshop was to increase awareness of the consequences that lifestyle choices, directly or indirectly, have on the ocular surface and adnexa. Several cross-sectional studies in the Lifestyle Challenges report2 found an association between depression and anxiety and DED symptoms, as well as the medications prescribed to treat the disorders.
The goal of the TFOS Lifestyle Workshop was to increase awareness of the consequences that lifestyle choices, directly or indirectly, have on the ocular surface and adnexa.
Anxiety and Stress
Individuals with depression may experience more intense dry eye symptoms and several pro-inflammatory cytokines have been found to be elevated in the tear fluid of individuals with depression. Although the evidence is weaker when it comes to DED signs, a Turkish study showed a lower tear break-up time (TBUT) and Schirmer score, and increased corneal staining in patients with depression and anxiety versus controls.3 The use of SSRIs have also been associated with lower Schirmer scores.
The pathophysiology between stress and DED is unknown, but psychological stress can increase systemic inflammatory activity, producing inflammatory cytokines, which may trigger ocular surface inflammation and may also affect pain perception. While stress and post-traumatic stress disorder (PTSD) have been associated with increased DED symptoms, there is little association with signs, although one study found poorer meibum expressivity associated with high stress levels.4 Both of our patients presented with meibomian gland dysfunction, requiring in-rooms heat and expression.
Sleep
Both the quantity and quality of sleep have been associated with DED symptoms – sleep deprivation can result in epithelial disruption, accumulation of lipid, morphological changes to microvilli, and a decrease in aqueous production.5 Resting after initial deprivation can reverse the changes. Reduced androgen levels, changes to circadian rhythms, decreased parasympathetic activity and brain-derived neurotrophic factor, and increased stress hormones from poor sleep quality can affect both lacrimal and meibomian gland disfunction and may be linked to DED. Interestingly, patients with Sjögren’s syndrome have more disturbed sleep and suffer more from sleep apnoea than controls, which may have been a particular trigger for Ms Bliht. There is some suggestion that patients who suffer with bad insomnia experience higher levels of ocular pain. Certainly Ms Jacob was suffering with intense ocular symptoms and slept poorly.
Cross-sectional studies have linked chronic pain conditions, such as irritable bowel syndrome, osteoarthritis, migraine, chronic pain syndrome, and fibromyalgia as risk factors for DED symptoms.1 Both our patients have a long history of IBS.
Nutrition
As the prevalence of nutrition-related chronic disease increases, it is important to understand the direct and indirect effects on the ocular surface – particularly as this is often a modifiable risk factor for DED.
The Nutrition report6 found macro and micro-nutrients are a source of energy that regulate the chemical processes of the body and are important in maintaining ocular health. Both systemic disorders and medications to treat them can change how the body processes nutrients. Changes in the gut biome may also lead to alterations on the ocular surface.
In mouse models, a high fat (associated with gut biome dysbiosis), high sugar, and highly processed food diet – similar to a Western diet – induced impaired aqueous production, goblet cell loss, corneal staining and disrupted the neuroimmune status of the cornea.7 The ratio of two main gut phyla – Firmicutes and Bacteroidetes – gives a rough guide to the state of gut dysbiosis. Gut dysbiosis has been related to systemic inflammatory diseases such as primary Sjögren’s syndrome, systemic lupus erythematosus, rheumatoid arthritis, B27-related disorders, IBS, graft versus host disease, and atopic disease.8 Imbalance of the gut microbiome has been associated with eye diseases such as uveitis, age-related macular degeneration, glaucoma, chalazion, and dry eye disease.
Many of these conditions are experienced by our patients, especially IBS. While there is no strong evidence to advise patients on the best dietary lifestyle to support DED, there is evidence that prebiotics and probiotics can improve the signs and symptoms of dry eye disease. The Mediterranean diet has been associated with a lower likelihood of developing primary Sjögren’s syndrome, and there is possible evidence that a 4:1 ratio of omega 3:6 is beneficial to DED signs, with a reduction of risk with every gram of omega 3 consumed, and even a suggestion that
omega 3 supplementation may offer neuroprotective effects on the cornea. There is strong evidence that vitamins A, B12, C, and D play a role in ocular surface health.
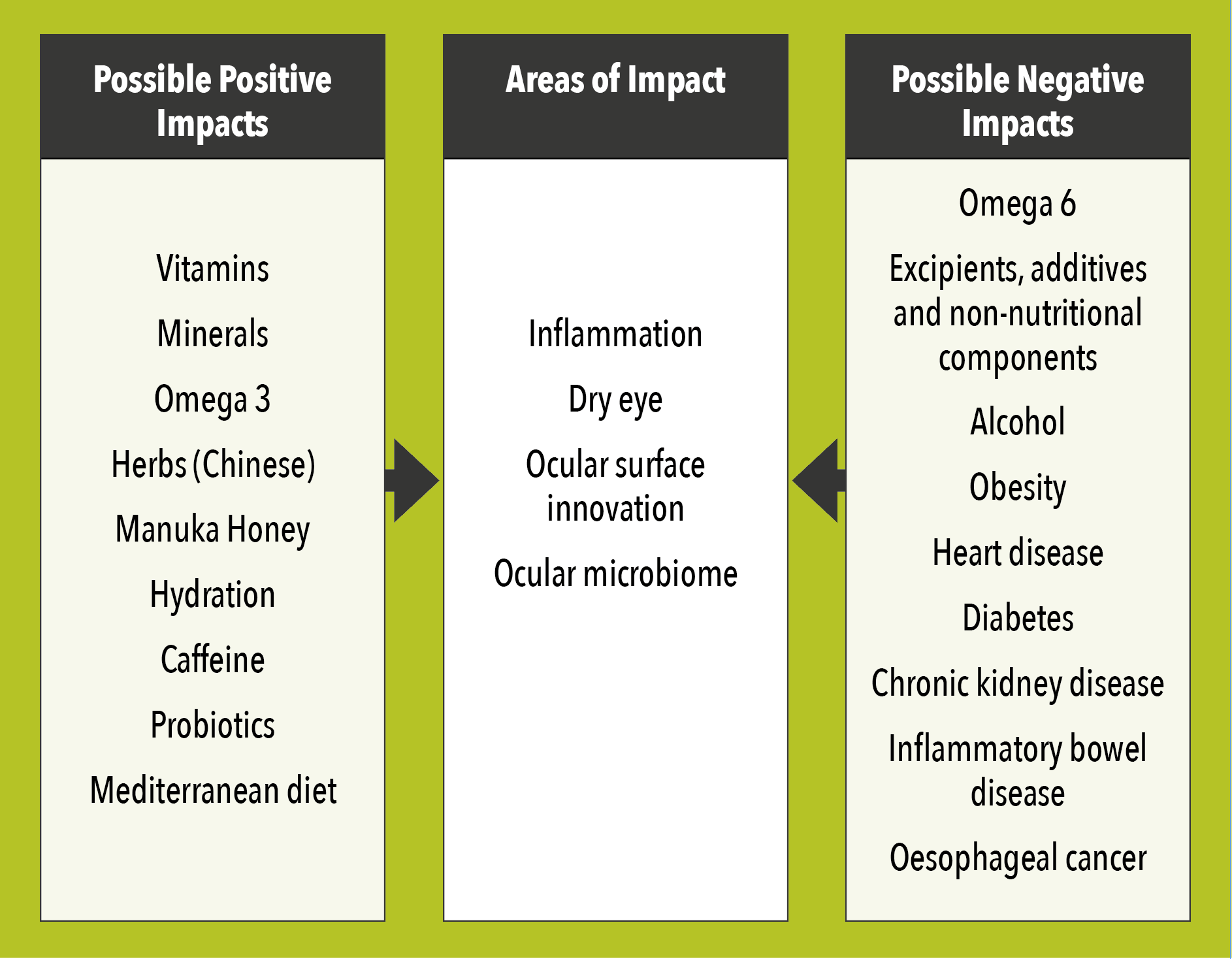
Figure 1. Summary of the possible positive and negative impacts on the ocular surface. Adapted from TFOS Lifestyle: Impact of nutrition on the ocular surface.6
Back to Our Patients
With Ms Jacob, it became quite clear that her recent pain from her pelvis, resultant poor sleep, and extreme stress, were likely culprits for her recent ocular symptoms, while her long history of thyroid imbalance, IBS and HRT may well have been her ‘why’ for DED. She decided to seek professional psychological support for her mental health, which made significant improvement to the way she managed both her stress and gut health, which in turn improved her DED symptoms. We decided on a further course of intense pulsed light therapy for longer ocular surface inflammation management, although she experienced intermittent styes as her stress levels changed during the course of treatment.
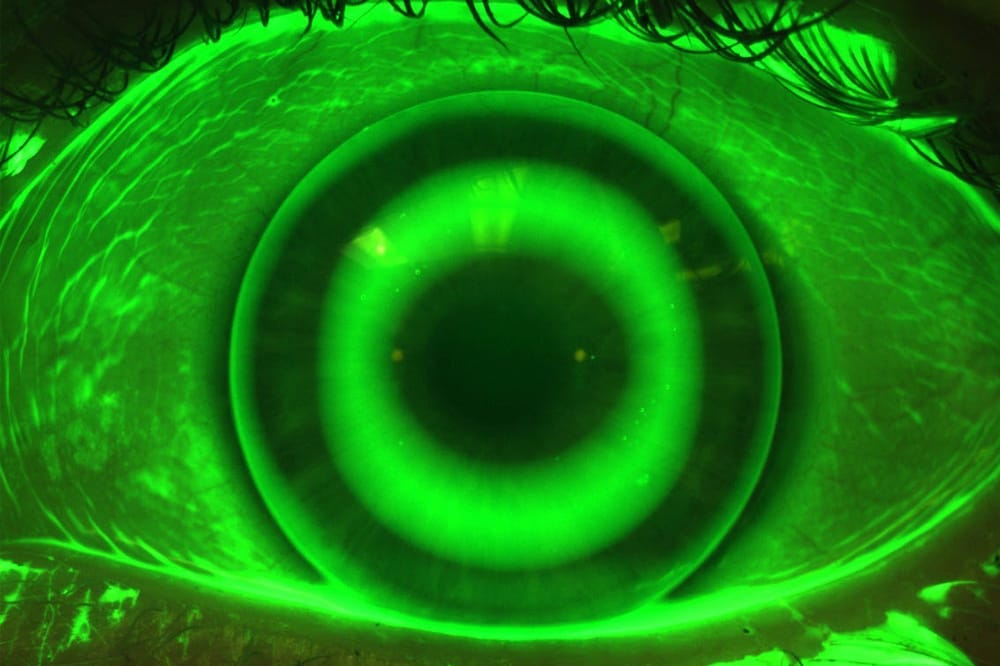
It would be easy to assume that Ms Bliht’s aqueous deficiency (Figure 1) was due to
both her use of SSRIs and Sjögren’s syndrome, but in light of the Lifestyle Challenges findings, factors such as her poor sleep patterns, depression, IBS, and chemotherapy may also have been contributing factors to her ‘why’, as well as her ongoing triggers. An altered ocular surface microbiome from her conjunctivitis may also have had a role in her MGD/dry eye development.9 We decided to use topical ciclosporin and she noted an improvement in her dry eye symptoms at her three-month review.
Building the Evidence
Much more research is needed to evaluate the role of lifestyle factors – for example, patients with chronic pain may also experience poor sleep patterns and anxiety or depression (Figure 2); they may have poor gut health associated with stress and a poor diet (Figure 3), along with other comorbidities.
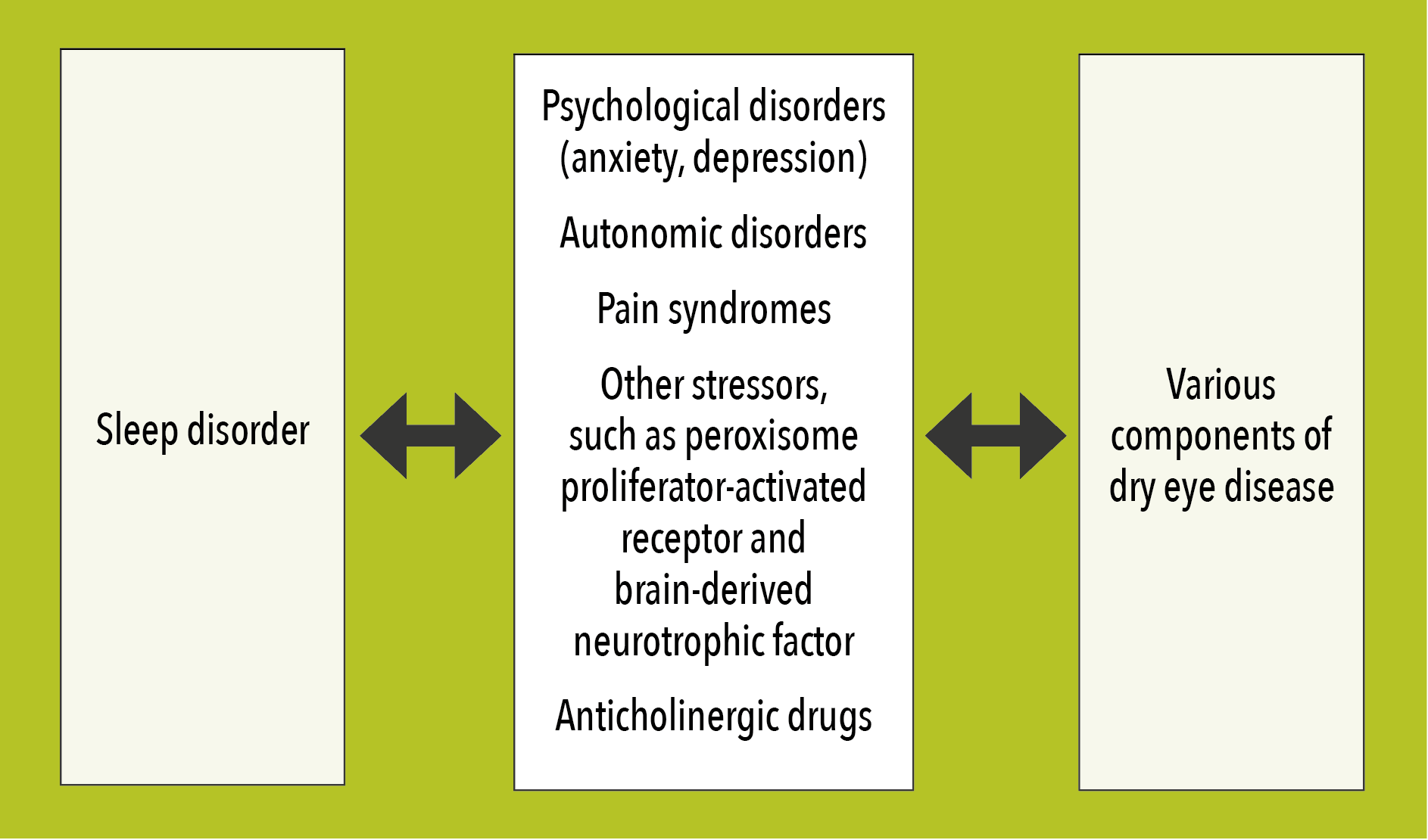
Figure 2. Potential mechanisms that my underline the association between sleep disorder and dry eye disease symptoms and signs. Adapted from TFOS Lifestyle: Impact of lifestyle challenges on the ocular surface.10
Figure 3. Ocular imaging indicates poor gut health associated with stress and a poor diet.
While there is no evidence yet to support patient education on these conditions, it is important to acknowledge the impact these risk factors may have on a patient’s DED, especially when not well controlled. This will help set expectations for the likelihood of successful management, and reaffirm the need to remain compliant with management regimes not only for their dry eye, but also for their lifestyle.
Knowledge of the impact of diet and lifestyle on DED will also help us understand the unexplained variation in a patient’s symptoms, or why they are not responding to treatments as expected.
*Patient names changed for anonymity.
Dr Jennifer Rayner BAppSc (Optom) GradCertOcTher (UNSW) was a registered nurse before studying optometry. She has practised as an optometrist since 2003 and with her business partner Dr Rene Malingre, established South Australia’s first dedicated dry eye clinic, Alleve Eye Clinic, in 2016. Dr Rayner is a committee member of the Tear Film and Ocular Society.
References
- Craig J, Alves M, Wolffsohn J, et al . TFOS Lifestyle Report executive summary: A lifestyle epidemic – ocular surface disease. The Ocular Surface. 2023 Oct 1;30:240–53. doi: 10.1016/j.jtos.2023.08.009.
- Galor A, Britten-Jones AC, Feng Y, et al. TFOS lifestyle: Impact of lifestyle challenges on the ocular surface. The Ocular Surface. 2023 Apr;28:262–303. doi: 10.1016/j.jtos.2023.04.008.
- Ulusoy MO, Işık-Ulusoy S, Kıvanç SA. Evaluation of dry eye disease in newly diagnosed anxiety and depression patients using anterior segment optical coherence tomography. Eye Vis (Lond). 2019 Aug 9;6:25. doi: 10.1186/s40662-019-0149-y.
- Wang MT, Muntz A, Wolffsohn JS, Craig JP. Association between dry eye disease, self-perceived health status, and self-reported psychological stress burden. Clin Exp Optom. 2021 Nov;104(8):835-840. doi: 10.1080/08164622.2021.1887580.
- Tang L, Wang X, Liu Z, et al. Sleep deprivation induces dry eye through inhibition of pparα expression in corneal epithelium. Invest Ophthalmol Vis Sci. 2018 Nov 1;59(13):5494-5508. doi: 10.1167/iovs.18-24504.
- Markoulli M, Arcot J, Caffery B, et al. TFOS lifestyle: Impact of nutrition on the ocular surface. The Ocular Surface. 2023 Apr 24;29. doi: 10.1016/j.jtos.2023.04.003.
- Bu J, Zhang M, Wu Y, Jiang N, Guo Y, He X, He H, Jeyalatha MV, Reinach PS, Liu Z, Li W. High-fat diet induces inflammation of meibomian gland. Investigative Ophthalmology & Visual Science. 2021 Aug 2;62(10):13-.
- Bajinka O, Tan Y, Abdelhalim KA, Özdemir G, Qiu X. Extrinsic factors influencing gut microbes, the immediate consequences and restoring eubiosis. Amb Express. 2020 Dec;10:1-1.
- Ozkan J, Majzoub ME, Willcox M, et al. Ocular microbiome changes in dry eye disease and meibomian gland dysfunction. Experimental Eye Research. 2023 Oct 1;235:109615. doi: 10.1016/j.exer.2023.109615.
- Galor A, Britten-Jones AC, Craig JP, et al. TFOS Lifestyle: Impact of lifestyle challenges on the ocular surface. Ocul Surf. 2023 Apr;28:262-303. doi: 10.1016/j.jtos.2023.04.008. Epub 2023 Apr 11. Erratum in: Ocul Surf. 2024 Apr;32:104. doi: 10.1016/j.jtos.2024.01.010.