
Strabismus, when first encountered by the novice health professional, can be very confusing. Perhaps some of the most confounding and even most hazardous aspects are the myths surrounding this condition. In this article, Dr Craig Donaldson AM sets out to debunk some of them.
Over the past 25 years I have had junior ophthalmic trainees refer to strabismology as the “dark art” and that “only sometimes does it make any sense at all”. Furthermore, the parent or carer of the affected child is often perplexed as to what is going on, making careful communication with explanation regarding their child’s condition imperative.
I will start by stating that strabismus is not a ‘dark art’ and in fact it is usually relatively straightforward. Indeed, the only two things holding the novice practitioner back are some knowledge and a little experience.
Strabismus, or misalignment of the eyes, affects up to 5% of the Australian population and as such, is one of the most common ocular conditions. Strabismus may be a primary or secondary disorder. The secondary disorders can be sight and /or life threatening. As such, coupled with the high incidence, it is important for health professionals and carers to have a solid understanding of the evaluation and diagnosis of strabismus. It is equally important to be aware of the misconceptions surrounding this condition.
…strabismus is not a ‘dark art’… the only two things holding the novice practitioner back are some knowledge and a little experience
The Myths
Myth 1. Ocular misalignment in young children is common and does not need to be evaluated.
Not only is this myth widespread, it is also very dangerous. Intermittent ocular misalignment in otherwise healthy children up to the age of three months is normal. This may manifest as an intermittent esotropia or exotropia. One large study of 1,219 healthy newborns found intermittent exotropia in 32.7% and esotropia in 3.2%.1 This is considered to be due to an immature oculomotor system. However, constant strabismus at any age and persisting strabismus beyond three months of age is never normal and warrants immediate formal assessment.
Immediate assessment is indicated because:
- The strabismus may be secondary to an important ocular, intracranial or systemic cause, and
- Strabismus is associated with a risk of developing amblyopia.
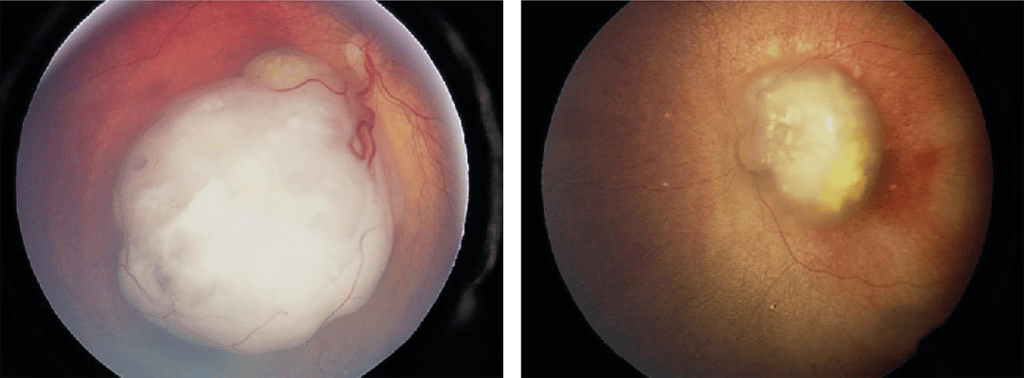
Figure 1. Two patients with retinoblastoma that presented with strabismus.
Ocular abnormalities that reduce vision can result in strabismus. These abnormalities comprise refractive error, ocular media opacities such as cataract and corneal scarring, and retinal disorders including retinoblastoma (retinal cancer) (Figure 1). After leukocoria, strabismus is the second most common presenting sign of retinoblastoma.2
Early diagnosis of retinoblastoma is crucial for globe salvage and the preservation of life. A review of 44 children who received no treatment revealed a 100% mortality within 48 months of diagnosis.3 With early diagnosis and therapy, retinoblastoma has a survival rate of over 99% in developed countries.4-6 It is also crucial to understand that retinoblastoma is a disease of young children and in our review of 67 affected patients from 2008–2018 at The Children’s Hospital at Westmead, New South Wales, the mean age of presentation was 9.2 months for bilateral disease and 23.5 months for unilateral disease.5
Intracranial causes of strabismus in young children are numerous and include cranial nerve palsies, cerebral palsy, hydrocephalus, brain tumours, and so on. A review of 206 patients diagnosed with strabismus in the first year of life showed 67% of patients with a constant exotropia and 49% of patients with esotropia had a coexisting ocular or systemic abnormality.7 Furthermore, smaller angles of deviation were associated with a higher likelihood of ocular or systemic abnormalities.
Refractive error, a refraction outside the expected normal for age, is associated with strabismus. Hypermetropia is typically associated with esotropia, and myopia more commonly associated with exotropia. Obversely, intermittent exotropia in children is also associated with a markedly increased risk of developing myopia. One study found an incidence of myopia of 90% in children diagnosed with intermittent exotropia over a 20-year period.8 Significantly, treatment of myopia should be commenced and indeed it is now the standard of care with the positions of the World Society Paediatric Ophthalmology and Strabismus,9 the World Council of Optometry,10 and Optometry Australia all aligned.11
The Sydney Paediatric Eye Disease Study found amblyopia in 1.9% of 2,461 examined children aged between six and 72 months from 2007 to 2009.12 Along with hypermetropia and ametropia, strabismus was identified as a major risk factor for amblyopia. Similar findings have been made in other large cohort studies from around the world.13-15
Clearly, strabismus in children requires evaluation, including cycloplegic refraction and dilated posterior segment examination. The myth that evaluation is not necessary is false and can lead to poor vision. In some cases it can be lethal.
Myth 2. Children will grow out of their strabismus.
As noted previously, infants aged under three months will often display an intermittent strabismus that resolves with maturation of the visual system.
Esotropia

Figure 2. Three patients with hypermetropia and accommodative esotropia.
The more common causes of esotropia in children include essential infantile esotropia, accommodative esotropia, acquired nonaccommodative esotropia (ANAET) of childhood, Duane syndrome, and sixth nerve palsy. Essential infantile esotropia occurs prior to six months of age and manifests as a large angle constant esotropia with typical clinical findings including full or almost full extraocular movements. Early onset esotropia in infants has been reported to resolve spontaneously, however this is uncommon and typically reported in those patients with a small angle variable misalignment.16-18 Patients with a constant esotropia >40 prism dioptres are very unlikely to resolve spontaneously.
Accommodative esotropia secondary to hypermetropia is often variable and tends to occur in children aged two to four years of age (Figure 2). While the refractive error remains untreated the esotropia is unlikely to resolve. Additionally, with time the risk of amblyopia increases, along with loss of binocular visual development.
ANAET is also associated with amblyopia and loss of binocularity. ANAET is a heterogenous group with a small but definite risk of intracranial pathology including intracranial neoplasm and hydrocephalus,19,20 and as such I routinely neuroimage children with this condition. Diplopia is relatively common and debilitating. The misalignment is unlikely to resolve spontaneously,21 and early surgical intervention is indicated to reestablish binocularity.
Duane syndrome is a congenital innervational movement disorder variably presenting as an esotropia or exotropia but consistently with globe retraction on attempted adduction. It is a hard-wired abnormality that does not resolve with time.
Sixth nerve palsy in children can rarely occur post-flu-like illness or vaccination and resolve spontaneously. Regardless, careful evaluation and possible investigation is always indicated in all cases of sixth nerve palsy in children, as sinister causes are not uncommon. One study reporting on 75 affected children found neoplasms associated with 45% and elevated intracranial pressure in 15%.22
Exotropia
The long-term follow-up of intermittent exotropia reveals that the deviation is unlikely to resolve spontaneously.23 One study of 184 paediatric patients with a mean follow-up of 9.2 years found that only five patients eventually resolved.24 Another reported a worsening of 75% of cases over 3.5-year follow-up.25
As mentioned previously, constant exotropia in infancy carries a significant risk of ocular, intracranial, and systemic abnormality. It is dangerous to assume that the exotropia will resolve, and immediate evaluation is imperative.
Vertical Strabismus
The causes of vertical strabismus in childhood includes, but are not limited to, fourth nerve palsy, dissociated vertical deviation (DVD) usually associated with infantile strabismus, Brown syndrome, monocular elevation deficiency, third nerve palsy, and trauma. Of these, Brown syndrome may show improvement with age. Brown syndrome is characterised by limitation of elevation in adduction and variable vertical deviation in the primary position secondary to an abnormality of the trochlear tendon complex. It has been variably found to resolve spontaneously in 10–68% of cases.26,27 Regardless, children with any of these conditions can develop amblyopia, significant abnormal head postures, and diplopia. The majority will not resolve spontaneously.
Not only are children unlikely to grow out of their strabismus but it is essential that they are evaluated to rule out critical underlying causes. Appropriate therapy must be commenced as soon as practicable to promote a favourable outcome visually and possibly systemically.
Myth 3. Small angles of strabismus are not as important as larger angles.
It is a common misconception that as far as strabismus is concerned, smaller angles are not as important as larger angles. Horizontal deviations of less than 10 prism dioptres are not readily noticeable and as such, it seems that satisfactory cosmetic appearance translates to the conclusion that such a misalignment is unimportant. In fact, this is not the case at all: small angles of strabismus can coincide with serious underlying pathology, profound amblyopia, and disabling diplopia. Significant, potentially amblyogenic refractive errors can present as a small variable ocular misalignment.
As mentioned previously, numerous intraocular and intracranial disorders can be associated with strabismus and the angle of deviation may be relatively small depending on the underlying pathology. For example, an incomplete sixth nerve palsy or intraocular tumour may present as a small angle horizontal strabismus. Indeed, research has found a greater incidence of ocular or systemic abnormalities with smaller, rather than larger, angles of misalignment.7
Microtropia (< 8 prism dioptres) is a reliable indicator of accompanying amblyopia.28 Longer occlusion and earlier institution of therapy has been found to be necessary for patients with microstrabismus.29,30 Additionally, worse initial vision acuity, later age of diagnosis, worse stereoacuity, and less occlusion therapy are all associated with a worse visual outcome.31,32 Children with larger angle strabismus may cross fixate, thus avoiding amblyopia.
Apart from the psychosocial impact of amblyopia, research has shown a real-life impact on educational, employment, and economic outcomes.33 Individuals with amblyopia are more likely to have hypertension, diabetes, and myocardial infarction.34 Furthermore, The Rotterdam Study35 showed that unilateral amblyopia more than doubled the lifetime risk of binocular visual impairment and other research has supported this conclusion.36
Children with early onset strabismus are usually spared the burden of diplopia due to the development of compensatory suppression. Despite this, acquired strabismus can certainly lead to diplopia and this can be disabling. The negative impact on educational, physical, and psychosocial development can be enormous. Additionally, a child presenting with diplopia is always a concerning clinical challenge. Serious underlying pathology must be necessarily ruled out and urgent assessment is indicated.
Clearly, the notion that small angles of strabismus are not as important as larger angles is incorrect and in some clinical conditions the opposite may actually be true.
Myth 4. Strabismus is only a cosmetic ailment.
That strabismus is ‘a cosmetic problem’ is certainly true for many affected patients and with this comes numerous psychological ramifications. The impact that strabismus has on the individual should not be underestimated. These include poor self-image, ridicule, social bias, isolation, and mental health issues,37,38 all of which are carried through to adulthood in untreated patients. People with strabismus are generally perceived as being less intelligent.39 Additionally, reduced employment and relationship opportunities have been reported.40
The idea that strabismus is only a cosmetic ailment can be taken in two ways. On one hand is the parent or carer who believes that it is a cosmetic problem, and that only, and as such it is not really very important. Often the comment is made that the child can decide on surgery when they get older. The numerous negative effects of strabismus on the growing child appear not to be readily understood. Sometimes this includes a fear of surgery or even spectacles.41 On the other hand is the parent or carer who sees cosmesis as the primary problem.
In both these scenarios, careful and understandable communication is imperative.
Essential infantile esotropia is associated with a delay in normal developmental milestones and early surgical correction has been shown repeatedly to produce a rapid improvement in gross motor skills.42 The re-establishment of stereopsis in acquired esotropia, resolution of diplopia in many types of strabismus, and improvement of head posture, can all be achieved in addition to cosmetic enhancement. A patient with a significant esotropia will have diminished peripheral binocular fields and this can also be rectified with appropriate treatment.
It is obvious that strabismus, although a cosmetic concern to many, covers a much greater range of different concerns. It is very important to recognise that strabismus therapy and surgery is reconstructive rather than cosmetic, and although strabismus has a substantial cosmetic component, the functional aspects are enormous.
… strabismus in children requires evaluation, including cycloplegic refraction and dilated posterior segment examination
Myth 5. Spectacles or patching will not be needed following strabismus surgery.
I am frequently asked whether the child will still require spectacles following strabismus surgery. Usually, the child is wearing their spectacles for a significant refractive error and rarely as a prism support to eliminate diplopia. With the latter situation, the goal of surgery is often to alleviate the need for prisms and so hopefully they will not be needed but as noted, this is a rare happening in children. The need for spectacles must be carefully explained to the parent or carer and patient, as otherwise disappointment and even annoyance may arise following successful surgery.
It can be puzzling for the guardian as to why both surgery and spectacles are necessary. It is important to explain the reasons in terms that are readily understandable to the lay person. As an example, one of the most common conditions causing confusion is partly accommodative esotropia with both a surgical and refractive component. I usually explain that children’s eyes turn abnormally inwards because they have either a focussing or a muscle problem, or sometimes both. The surgery addresses the muscle issue and the spectacles the focussing issue. If spectacles alone align the eyes, then it is purely a focussing issue and surgery is not indicated. This is usually understood and accepted.
As well, it is essential that the carer is educated regarding the role of vision development in the first decade. Patching may remain an important part of therapy following strabismus surgery if amblyopia persists or if it develops.
Myth 6. Strabismus surgery can only be performed once.
I am not sure how this myth arose. It is typically mentioned by a parent who underwent strabismus surgery themselves, somewhat unsuccessfully, and they or their parents were told that no further surgery should be performed. I suspect that if the message given to them was correct, then it reflected more the abilities of the attending eye surgeon rather than a clinical justification.
Strabismus surgery remains a somewhat inexact science as the results can be variable. The reason for this relates to variable eye muscle surgery dose response from person to person, variable healing, difficulty in measuring the angle of the deviation in young children, and that some conditions develop other movement disorders with time. The classic example of this is essential infantile esotropia where patients presenting with an esotropia have a relatively high chance of later developing other problems, such as inferior oblique overaction and dissociated vertical deviation.
I have personally encountered an adult patient who calmly informed me that during her life she had had 21 strabismus surgeries, and she had the records to prove her story. Her 22nd surgery seemed to do the trick. I believe that available techniques, such as adjustable sutures, are a very helpful tool in patients requiring further surgery. Adjustable suture surgery is generally performed outside childhood owing to part of the surgery being performed under topical anaesthetic with the patient awake. This is clearly a very extreme example, but it does help dispel the myth.
Myth 7. Strabismus surgery carries a high risk of permanent diplopia.
Diplopia is certainly a well-recognised possible complication of surgery. Every patient, no matter the age, should be counselled regarding the same. Fortunately, it is very uncommon and less likely to occur in children who have, or are able to develop, suppression of the second image. It is rare for adults who have not previously had diplopia to develop it following strabismus surgery.43-45 One study reported diplopia in 9% of patients in the first six weeks after surgery, however all but 0.8% reolved.46
Diplopia is more likely to arise with overcorrections when the eye is moved away from its field of suppression. A child with an exotropia who has developed temporal hemifield suppression may well experience diplopia if their eyes are overcorrected to esotropia.
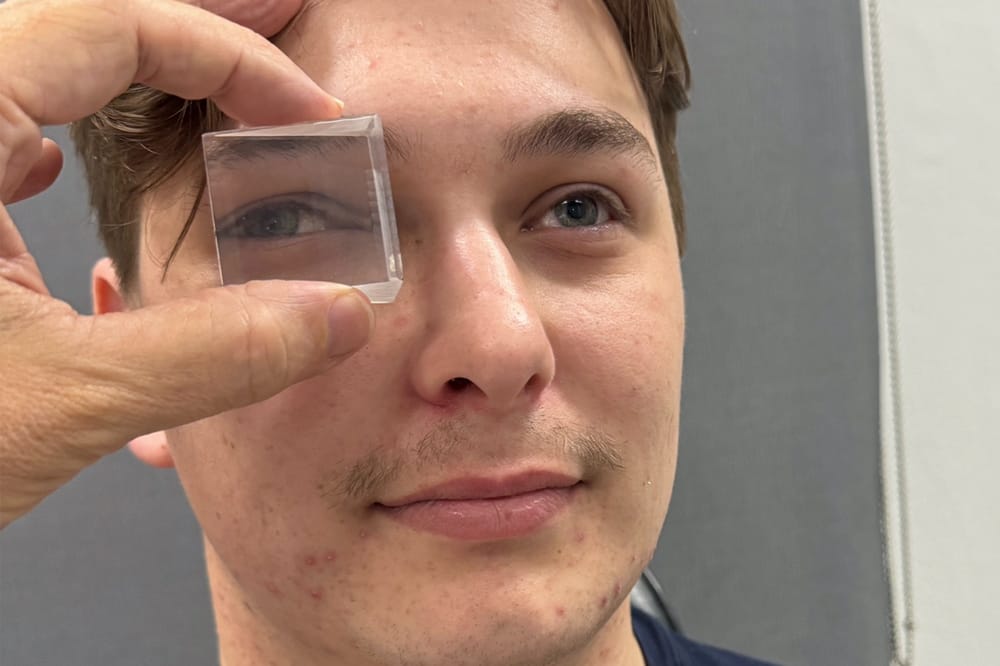
The risk of post-operative diplopia is greater in patients who have pre-operative diplopia that cannot be neutralised with prisms. In older patients, I routinely used free prisms in space. This very simply involves neutralising the angle of the strabismus by holding prism(s) in front of the patient’s eyes and asking them whether diplopia is perceived when looking at an object at six metres and also at near (Figure 3, see main image above). If diplopia is noted, then the patient must be advised that post-operative diplopia may occur. Again, adjustable sutures may aid in decreasing the chance of this happening.
Myth 8. Children with strabismus have no depth perception.
While it is true that it is not possible for patients with a constant strabismus to have normal stereovision, they still possess a degree of depth perception. This is obtained by using clues such as image size, surrounding items, object movement, and shading. A monocular patient will also have a degree of depth perception in the same way. This is easily demonstrated to parents clinically by, for example, holding two toys at different distances and asking the child which object is closer or further away from them.
Some patients who undergo successful surgical realignment will achieve normal stereo vision. The outcome varies depending on the underlying condition. For example, normal stereo vision is more likely to occur in those that have previously had normal alignment such as ANAET, and less likely in those with essential infantile esotropia.46,47
Summary
Strabismus can be a confusing condition. Numerous myths have arisen regarding strabismus, and these are founded in misunderstandings and misinformation. These myths can lead to delay or deprivation of essential evaluation and management. In the worst-case scenario, a child’s life could be lost due to critical underlying pathologies. Among other outcomes, a child may endure lifelong disability including reduced vision, diplopia, decreased self-esteem, and reduced opportunities. It is crucial that the eye care health professional understands the facts of childhood strabismus and that they take their time to carefully and fully educate, reassure, and treat the patient as well as the parental concerns.
To earn your CPD hours from this article visit: mieducation.com/paediatric-strabismus-exploring-eight-myths.

Dr Craig Donaldson
Dr Craig Donaldson AM MBBS FRANZCO FRACS completed the Sydney Eye Hospital training program before undertaking strabismus and paediatric ophthalmology fellowship training at Hospital for Sick Children in Toronto, Canada. Dr Donaldson is a senior staff specialist at The Children’s Hospital at Westmead, a VMO at Sydney Eye Hospital and Sydney Children’s Hospital, and head of the Strabismus and Paediatric Unit at Sydney Eye Hospital. From 2012–2018 he was president of the Australian and New Zealand Strabismus Society. He is RANZCO NSW State Branch Treasurer and a Federal Councillor. Dr Donaldson has authored numerous journal articles, book chapters and lectured extensively in Australia and internationally.
In 2019 he was awarded a Member of the Order of Australia (AM) for services to ophthalmology and medicine and the APAO prevention of blindness award in Asia.
References
- Nixon RB, Helveston EM, Ellis FD, et al. Incidence of strabismus in neonates. Am J Ophthalmol. 1985 Dec 15;100(6):798-801. doi: 10.1016/s0002-9394(14)73370-7.
- Kiernan M, Fabian ID, Reddy MA, et al. Strabismus as a presenting sign in retinoblastoma. J Pediatr Ophthalmol Strabismus. 2021 Sep-Oct;58(5):324-330. doi: 10.3928/01913913-20210614-03.
- Zhao J, Feng Z, Gallie BL. Natural history of untreated retinoblastoma. Cancers (Basel). 2021 Jul 21;13(15):3646. doi: 10.3390/cancers13153646.
- Global Retinoblastoma Study Group. The Global Retinoblastoma Outcome Study: a prospective, cluster-based analysis of 4064 patients from 149 countries. Lancet Glob Health. 2022 Aug;10(8):e1128-e1140. doi: 10.1016/S2214-109X(22)00250-9.
- Starte J, Taher A, Powys M, Donaldson C, Jones, M, et al. Management and outcomes of retinoblastoma cases presenting to Children’s Hospital Westmead, Sydney between 2008 and 2018. International Journal of Ophthalmology and Visual Science. 2021;6:273-280. doi: 10.11648/j.ijovs.20210604.24.
- Berman EL, Donaldson CE, Giblin M, Martin FJ. Outcomes in retinoblastoma, 1974–2005: The Children’s Hospital, Westmead. Clin Exp Ophthalmol. 2007 Jan-Feb;35(1):5-12. doi: 10.1111/j.1442-9071.2006.01386.x.
- Hunter DG, Ellis FJ. Prevalence of systemic and ocular disease in infantile exotropia: Comparison with infantile esotropia. Ophthalmology. 1999 Oct;106(10):1951-6. doi: 10.1016/S0161-6420(99)90407-4.
- Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. The development of myopia among children with intermittent exotropia. Am J Ophthalmol. 2010 Mar;149(3):503-7. doi: 10.1016/j.ajo.2009.10.009.
- World Society of Paediatric Ophthalmology and Strabismus, Myopia Consensus Statement 2023, available at: wspos.org/swdcore/uploads/WSPOS-Myopia-Consensus-Statement-2023-1.pdf [accessed Nov 2024].
- World Council of Optometry, Resolution: The Standard of Care for Myopia Management by Optometrists, available at: worldcouncilofoptometry.info/resolution-the-standard-of-care-for-myopia-management-by-optometrists/ [accessed Nov 2024].
- Optometry Australia. Position Statement on Myopia Management [Internet]. 2024. Available at: optometry.org.au/wp-content/uploads/Professional_support/Guidelines/Myopia-Position-Statement-2024-v2.pdf [accessed Oct 2024].
- Pai AS, Rose KA, Mitchell P, et al. Amblyopia prevalence and risk factors in Australian preschool children. Ophthalmology. 2012 Jan;119(1):138-44. doi: 10.1016/j.ophtha.2011.06.024.
- Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages six to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008 Jul;115(7):1229-1236.e1. doi: 10.1016/j.ophtha.2007.08.001.
- Chia A, Dirani M, Saw SM, et al. Prevalence of amblyopia and strabismus in young Singaporean Chinese children. Invest Ophthalmol Vis Sci. 2010 Jul;51(7):3411-7. doi: 10.1167/iovs.09-4461.
- Matsuo T, Matsuo C, Matsuoka H, Kio K. Detection of strabismus and amblyopia in 1.5- and 3-year-old children by a preschool vision-screening program in Japan. Acta Med Okayama. 2007 Feb;61(1):9-16. doi: 10.18926/AMO/32910.
- Pediatric Eye Disease Investigator Group. Spontaneous resolution of early-onset esotropia: experience of the Congenital Esotropia Observational Study. Am J Ophthalmol. 2002 Jan;133(1):109-18. doi: 10.1016/s0002-9394(01)01316-2.
- Birch E, Stager D, Wright K, Beck R. The natural history of infantile esotropia during the first six months of life. Pediatric Eye Disease Investigator Group. J AAPOS. 1998 Dec;2(6):325-8; discussion 329. doi: 10.1016/s1091-8531(98)90026-x.
- Pasrons L. Spontaneous resolution of early onset esotropia: Two case studies. Australian Orthoptic Journal 2010 Vol 42(2). Orthoptics Australia.
- Mohney BG. Acquired nonaccommodative esotropia in childhood. J AAPOS. 2001 Apr;5(2):85-9. doi: 10.1067/mpa.2001.113313.
- C Simon JW, Waldman JB, Couture KC. Cerebellar astrocytoma manifesting as isolated, comitant esotropia in childhood. Am J Ophthalmol. 1996 May;121(5):584-6. doi: 10.1016/s0002-9394(14)75442-x.
- Jacobs SM, Green-Simms A, Diehl NN, Mohney BG. Long-term follow-up of acquired nonaccommodative esotropia in a population-based cohort. Ophthalmology. 2011 Jun;118(6):1170-4. doi: 10.1016/j.ophtha.2010.10.032.
- Lee MS, Galetta SL, Volpe NJ, Liu GT. Sixth nerve palsies in children. Pediatr Neurol. 1999 Jan;20(1):49-52. doi: 10.1016/s0887-8994(98)00090-3.
- Zhang KK, Koklanis K, Georgievski Z. Intermittent exotropia: A review of the natural history and non-surgical treatment outcomes. Australian Orthoptic Journal 2007: Vol 39 (1).
- Nusz KJ, Mohney BG, Diehl NN. The course of intermittent exotropia in a population-based cohort. Ophthalmology. 2006 Jul;113(7):1154-8. doi: 10.1016/j.ophtha.2006.01.033.
- von Noorden GK, Campos EC. Binocular vision and ocular motility: Theory and management of strabismus. St Louis, USA: Mosby Year Book Inc, 2002.
- Rodrigues P, Seldon R, Varandas G, Vieira M. (2018) Natural history and treatment of Brown’s Syndrome: Long-term experience. Open Journal of Ophthalmology. 08. 232-240. doi: 10.4236/ojoph.2018.84027.
- Kaban TJ, Smith K, Cadera W, et al. Natural history of presumed congenital Brown Syndrome. Arch Ophthalmol. 1993;111(7):943-946. doi: 10.1001/archopht.1993.01090070061020.
- Lysons D, Tapley J. Is microtropia a reliable indicator of the presence of amblyopia in anisometropic patients? Strabismus. 2018 Sep;26(3):118-121. doi: 10.1080/09273972.2018.1503308.
- Utamura K, Wakayama A, Kusaka S et al. Factors affecting the total occlusion time in eyes with hyperopic anisometropic amblyopia. BMC Ophthalmol. 2023 Nov 20;23(1):469. doi: 10.1186/s12886-023-03206-7.
- Matsuo T, Kawaishi Y, Watanabe Y, et al. Long-term visual outcome in primary microtropia. Jpn J Ophthalmol. 2003 Sep-Oct;47(5):507-11. doi: 10.1016/s0021-5155(03)00105-9.
- Stewart CE, Fielder AR, Stephens DA, Moseley MJ. Treatment of unilateral amblyopia: factors influencing visual outcome. Invest Ophthalmol Vis Sci. 2005 Sep;46(9):3152-60. doi: 10.1167/iovs.05-0357.
- Hong J, Kuo D, Su H, Li L, Guo Y, Chu H, Fu J. Ocular and visual perceptive factors associated with treatment outcomes in patients with anisometropic amblyopia. BMC Ophthalmol. 2023 Jan 12;23(1):21. doi: 10.1186/s12886-023-02770-2.
- Bountziouka V, Cumberland PM, Rahi JS. Impact of persisting amblyopia on socioeconomic, health, and well-being outcomes in adult life: Findings from the UK Biobank. Value Health. 2021 Nov;24(11):1603-1611. doi: 10.1016/j.jval.2021.05.010.
- Wagner SK, Bountziouka V, Hysi P, Rahi JS; UK Biobank Eye and Vision Consortium. Associations between unilateral amblyopia in childhood and cardiometabolic disorders in adult life: A cross-sectional and longitudinal analysis of the UK Biobank. EClinicalMedicine. 2024 Mar 7;70:102493. doi: 10.1016/j.eclinm.2024.102493.
- van Leeuwen R, Eijkemans MJ, Simonsz HJ, et al. Risk of bilateral visual impairment in individuals with amblyopia: the Rotterdam study. Br J Ophthalmol. 2007 Nov;91(11):1450-1. doi: 10.1136/bjo.2006.113670.
- Rahi J, Logan S, Timms C, Russell-Eggitt I, Taylor D. Risk, causes, and outcomes of visual impairment after loss of vision in the non-amblyopic eye: a population-based study. Lancet. 2002 Aug 24;360(9333):597-602. doi: 10.1016/s0140-6736(02)09782-9.
- Buffenn AN. The impact of strabismus on psychosocial heath and quality of life: a systematic review. Surv Ophthalmol. 2021 Nov-Dec;66(6):1051-1064. doi: 10.1016/j.survophthal.2021.03.005.
- Kothari M, Balankhe S, Gawade R, Toshnival S. Comparison of psychosocial and emotional consequences of childhood strabismus on the families from rural and urban India. Indian J Ophthalmol. 2009 Jul-Aug;57(4):285-8. doi: 10.4103/0301-4738.53053.
- Mojon-Azzi SM, Kunz A, Mojon DS. The perception of strabismus by children and adults. Graefes Arch Clin Exp Ophthalmol. 2011 May;249(5):753-7. doi: 10.1007/s00417-010-1555-y.
- Hatt SR, Leske DA, Holmes JM, et al. The effects of strabismus on quality of life in adults. Am J Ophthalmol. 2007 Nov;144(5):643-7. doi: 10.1016/j.ajo.2007.06.032.
- Al-Omari R, Jammal HM, Khatatbeh M, et al. Adults with longstanding strabismus: Psychosocial and functional impacts and reasons behind surgery delay. J Ophthalmol. 2022 Jun 16;2022:8682675. doi: 10.1155/2022/8682675.
- Drover JR, Stager DR Sr, Birch EE, et al. Improvement in motor development following surgery for infantile esotropia. J AAPOS. 2008 Apr;12(2):136-40. doi: 10.1016/j.jaapos.2007.08.013.
- Kushner BJ. Intractable diplopia after strabismus surgery in adults. Arch Ophthalmol. 2002 Nov;120(11):1498-504. doi: 10.1001/archopht.120.11.1498.
- Wang JY, Leske DA, Hatt SR, Holmes JM. Diplopia after strabismus surgery for adults with nondiplopic childhood-onset strabismus. J AAPOS. 2019 Dec;23(6):313.e1-313.e5. doi: 10.1016/j.jaapos.2019.07.005.
- Coats D. Persistent diplopia following surgery. In: Strabismus surgery and its complications. (Springer, Berlin, Heidelberg, 2007). Doi: 10.1007/978-3-540-32704-2_31.
- Birch EE, Wang J. Stereoacuity outcomes after treatment of infantile and accommodative esotropia. Optom Vis Sci. 2009 Jun;86(6):647-52. doi: 10.1097/OPX.0b013e3181a6168d.
- Tychsen L. Can ophthalmologists repair the brain in infantile esotropia? Early surgery, stereopsis, monofixation syndrome, and the legacy of Marshall Parks. J AAPOS. 2005 Dec;9(6):510-21. doi: 10.1016/j.jaapos.2005.06.007.





