Successful cataract and refractive surgery begins well before the patient enters the operating theatre. As the eye’s first refractive surface, the tear film is critical for accurate biometry, clear intraoperative visualisation, and ultimately, surgical outcomes and patient satisfaction.1 Even subtle tear film instability can compromise preoperative measurements, increase the risk of refractive surprises, and diminish surgical outcomes.
In this article, ophthalmologist Dr Darian-Smith and optometrist Dr Margaret Lam discuss the benefits of collaboration between the professions ahead of surgery.
LEARNING OBJECTIVES
On completion of this CPD activity, participants should:
- Understand the prevalence of dry eye disease, particularly in surgical candidates,
- Realise the importance of early detection and intervention to optimise the tear film ahead of cataract and refractive surgery,
- Be prepared to proactively screen for dry eye, and
- Understand the need for ongoing collaborative care pre- and postocular surgery to improve patient outcomes.
A substantial proportion of surgical candidates present with clinical signs of dry eye disease (DED) yet remain asymptomatic. If left undetected, these patients face an increased likelihood of suboptimal surgical outcomes, postoperative discomfort, and dissatisfaction – even when the surgical procedure itself is technically successful.2
Addressing these challenges requires a proactive, collaborative approach. Optometrists, as the first point of contact for many patients, are well placed to detect and initiate tear film optimisation at the time of referral. Ophthalmologists, in turn, can build on these early interventions to reduce surgical delays, improve the reliability of biometric data, and ultimately enhance patient outcomes, satisfaction, and trust.
By working in partnership – integrating early identification, targeted optimisation, and coordinated post-surgical care – optometrists and ophthalmologists can deliver more predictable results, streamline the surgical pathway, and elevate the overall standard of patient care. Together, they can ensure that every patient enters surgery with a healthy, optimised tear film – optimising both surgical outcomes and patient experiences.
Why Preoperative Tear Film Management Matters
Dry eye disease is highly prevalent, affecting 5–50% of the population and up to 63% in some groups, depending on diagnostic criteria and risk factors.3,4 Its impact spans both older cataract patients and younger refractive candidates. For many, contact lens intolerance driven by DED is a common reason for seeking laser vision correction, while surgical procedures themselves can also induce or exacerbate dry eye symptoms.5
Studies show that up to 80% of cataract patients present with at least one sign of ocular surface dysfunction prior to surgery, while preoperative symptoms have been reported in 38% of laser-assisted in situ keratomileusis (LASIK) and 48% of photorefractive keratectomy (PRK) patients in the refractive surgery population.6-10 Importantly, a large proportion of patients remain asymptomatic despite clinical indication of disease.6,8,11
With approximately 250,000 cataract procedures and thousands of refractive surgeries performed each year in Australia, proactive screening and optimisation of the tear film should be prioritised in practice.12-15 Clinicians may assume a reasonable probability of ocular surface disease – even when patients deny symptoms – making routine surface screening essential.5,6,16 Untreated DED in both symptomatic and asymptomatic patients can compromise preoperative measurements, reduce postoperative comfort, and may ultimatel be the difference between a technically successful or truly satisfactory surgery.2,5,17
Impact on Biometry Measurements and Post-Op Results
The precorneal tear film plays a pivotal role in the eye’s total refractive power, and even subtle instability can affect the accuracy of preoperative biometry.18 Whether planning cataract extraction, refractive procedures such as LASIK or PRK, or premium intraocular lens (IOL) implantation, precise preoperative measurements are essential for achieving optimal surgical outcomes. Tear film instability can:17-21
- Distort corneal power measurements and topography, leading to variable keratometry readings,
- Undermine IOL calculations, increasing the risk of postoperative refractive surprises – specifically, it can change the toricity of a lens and the axis of astigmatism, which can greatly impact on the final refractive outcome,
- Result in poor or fluctuating visual quality and, ultimately,
- Lower patient satisfaction, even when the surgery itself is technically successful.
As modern patients’ expectations increase, both preoperative tear film optimisation and ongoing postoperative maintenance have become integral to the surgical journey.
Achieving these outcomes requires close collaboration between optometrists and ophthalmologists, with optometrists playing a proactive role in early detection, management, and patient education. By prioritising tear film stability at every stage, clinicians can help ensure both the technical and experiential success of ocular surgery.
Preoperative Dry Eye Diagnosis and Management
Meeting patients’ high expectations for visual outcomes following surgery means addressing ocular surface disease before surgery. Optometrists are uniquely positioned to initiate optimisation of the ocular surface, supporting ophthalmologists in accurate surgical planning and enhancing patient satisfaction.
DED is multifactorial and can be challenging to manage but a systematic, evidence-based approach streamlines care. The TFOS DEWS II and III reports remain the gold standard, providing clear frameworks for both diagnosis and management.22-24
Practical preoperative screening tools include:22
- Symptom questionnaire: Ocular Surface Disease Index (OSDI-6) (score ≥4)
- Non-invasive tear break-up time (NITBUT): <10 seconds,
- Tear film osmolarity: ≥308 mOsm/L in either eye or interocular difference >8 mOsm/L,
- Ocular surface staining: >5 corneal fluorescein spots, >9 conjunctival lissamine green spots, or lid margin staining ≥2 mm length and ≥25% width.
A diagnosis is typically based on a positive symptom score plus at least one abnormal objective test (NITBUT, osmolarity, or staining). However, as many patients may exhibit significant ocular surface signs without symptoms, it is still recommended that these cases are managed proactively.22 It is also important to consider that heavy contact lens use can cause the cornea to become neuropathic to an extent, reducing the severity and type of symptoms that a patient may experience – even if clinical signs point towards moderate to severe ocular surface disease.
Practical Guidance on Preoperative Management
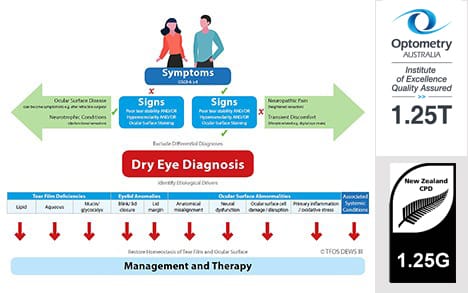
The results of a thorough dry eye evaluation are paramount in guiding treatment decisions before surgical referral. The updated TFOS DEWS III Management and Therapy report shifts the focus from a staged approach to achieving specific treatment goals, offering algorithms based on the clinically relevant drivers (Figure 1) of each patient’s condition.23,24

Figure 1. Dry eye disease management and therapy.22
Subclassification and Targeted Management23,24
DED Subtypes. TFOS DEWS II and III emphasise subclassifying DED into aqueous-deficient (ADDE), evaporative (EDE), or mixed forms. Evidence suggests that approximately two-thirds of patients present with EDE.
Expanded Drivers. The latest TFOS DEWS III report recognises a broader spectrum of aetiological drivers – including tear film deficiencies, eyelid anomalies, and ocular surface abnormalities – requiring tailored diagnostic and therapeutic strategies (Figures 2–4).



Tailored Therapy. Distinguishing the dominant driver is critical for selecting effective interventions and optimising patient outcomes.
Management Principles23-24
- Preservative-free artificial tears (AT) remain a cornerstone of evidence-based DED management, providing tear supplementation and stabilisation.
- Lifestyle modifications and meibomian gland function optimisation are essential adjuncts.
- Concurrent management of multiple deficiencies is often necessary, as dry eye subtypes frequently overlap.
Use of Cationorm
When choosing an AT, an option to consider is Cationorm (CSL Seqirus). Cationorm is a preservative-free oil-in-water AT for DED that uses cationic emulsion (CE) technology.25 The unique formulation, with its positive-charge, is designed to be attracted to the negatively-charged ocular surface, optimising spread and residence time on the ocular surface without compromising on viscosity (Figure 5A).25 Unlike many other ATs, Cationorm targets all layers of the tear film (Figure 5B) and is suitable for the different subtypes of dry eye disease including evaporative, aqueous deficient and mixed.25-28
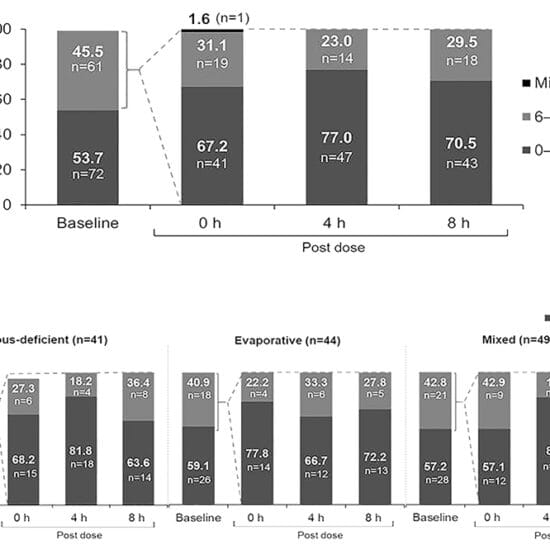
The efficacy of Cationorm for the treatment of DED has been demonstrated in several randomised, controlled, multicentre clinical trials.25,29-31 Evidence has also highlighted its specific value in the early postoperative period following refractive surgery, when tear film instability is common and recovery depends on ocular surface optimisation.
- In a study of 80 post-LASIK patients, Cationorm demonstrated significantly greater improvements in tear break-up time (TBUT) and patient-reported symptoms (dryness, irritation, burning) compared with Systane Ultra, with benefits evident by day 15 and maintained at one month.32
- In 129 patients undergoing transPRK or Epi-Bowman keratectomy (EBK), Cationorm was superior to 0.15% sodium hyaluronate for improving
OSDI scores at both one week and one month. Patients using Cationorm also reported significantly less blurred vision after drop instillation.33
Together, these findings support Cationorm, not only as an effective treatment for DED in general, but also as a valuable choice for DED both before and after surgery to optimise tear film stability and support surgical recovery.
Case Study: Dr Darian-Smith
Prior to refractive lens replacement or laser eye surgery, all patients at Eagle Eye Surgeons are optimised for surgery, with an important focus on dry eye for which we provide a comprehensive suite of treatments.
Even those that do not have considerable ocular surface disease need treatment prior to surgery for accurate diagnostic scanning. This is in the form of preservative free lubrication four times daily for a period of two to four weeks prior to surgery. Our preferred preservative free lubricant is Cationorm as it is effective in treating both evaporative and aqueous deficiency subtypes of dry eye. We couple this with Lacritec (Stiltec) for Omega 3 supplementation. In cases with pre-existing ocular surface disease, generally in heavy contact lens wearers, we add an addition of topical steroid such as FML (fluorometholone, AbbVie) four times daily for a month prior in a weaning dosage.
The benefits of priming our refractive patients with a preservative free lubricant such as Cationorm are numerous:
- The accuracy of keratometry readings on both corneal tomography and optical coherence tomography (OCT) devices (Pentacam and MS39) and biometry (IOL Master 700) are greatly improved. This affects the type of lens being inserted into the eye or, specifically for laser refractive surgery, the accuracy of the refraction being inputted into the laser.
- Postoperative comfort and prevention of the development of worsening dry eye after surgery. After surgery for both lens and refractive laser patients, preservative free lubricants are continued for a few months to aid with tear film regeneration. We couple this with custom-made preservative-free topical postoperative steroids and antibiotics. The tear film usually reverts to its preoperative baseline approximately six to eight weeks after surgery, so it is essential that lubrication continues until this disruption is restored.
A 52-year-old female was seen at our practice. She was undergoing assessment for suitability for Presbyond laser eye surgery, a type of refractive LASIK procedure combining the principles of optimisation of spherical aberrations coupled with micro-anisometropia, designed to remove the need for glasses for both distance and near.
She was a heavy soft daily contact lens wearer for many years. Contacts were removed for a period of five days prior to the initial assessment. She was found to have a rapid TBUT (eight seconds) and mild aqueous deficiency dry eye with inferior superficial punctate epithelial erosions (SPEEs) 4–5. She was a low hyperope with presbyopia. A contact lens holiday was initiated, and the patient was asked to use Cationorm four times daily for a month, coupled with Lacritec. The patient returned four weeks later with a change in her prescription and importantly, a change in the axis of her astigmatism – the mild-moderate preoperative dry eye which was most likely contact lens induced had resolved with a tear film of 14 seconds and complete absence of SPEEs. The patient was booked for surgery, and the refraction was repeated on the day of surgery with no changes. The patient underwent routine bilateral Presbyond laser surgery. At the one week review she was 6/4.8-2 and J2 in both eyes. Despite undergoing LASIK, the preoperative drop regimen was continued for a period of eight weeks. The patient did not experience any discomfort or symptoms of ocular surface dysfunction. This case highlights the importance of preoperative optimisation of the ocular surface to ensure stability and accuracy of refractions, and also to ensure a safe laser outcome for our patients.
Conclusion
In summary, dry eye disease is common and potentially often underdiagnosed in surgical candidates. Proactive screening and management by optometrists – using evidence-based frameworks and close collaboration with ophthalmologists – are essential for optimising the tear film, improving surgical accuracy, and enhancing patient satisfaction. Early intervention and coordinated care set the foundation for successful outcomes in cataract and refractive surgery. And finally, while ocular surface optimisation upfront is critical, maintenance following the procedure remains equally vital.
Referral Checklist: Ocular Surface Optimisation and Continuum of Care |
|---|
For Optometrists (Pre-Referral) Screen every surgical candidate for DED, regardless of symptoms. Perform baseline testing (symptom questionnaire and at least one objective test: NITBUT, osmolarity, staining). Identify exacerbating factors (contact lens overwear, systemic medications, environment). Initiate targeted management (artificial tears, lid hygiene, meibomian gland optimisation, lifestyle changes). Consider artificial tears that target all layers of the tear film and preservative-free options to minimise corneal toxicity (e.g. Cationorm) and prescribe any other appropriate treatments, for example, warm compresses and Omega 3 supplementation. Allow six to eight weeks of therapy prior to biometry, where possible. Confirm ocular surface stability and readiness for referral for consideration for surgery. For Ophthalmologists (At Referral and Pre-Surgery) Review and build on optometrist’s optimisation plan. Repeat/verify key surface tests before biometry. Delay surgery if significant instability remains. Discuss expectations with patient regarding DED management. For Shared Postoperative Care Continue artificial tear/lid hygiene regimen post-surgery. Monitor for exacerbation of DED symptoms. Escalate therapy if recovery is delayed or symptoms worsen. Maintain ongoing co-management for chronic dry eye. |
This article is sponsored by CSL Seqirus. Drs Erica Darian-Smith and Margaret Lam were paid an honorarium by CSL Seqirus to author this article.
 Dr Erica Darian-Smith MBBS MMed GradDipRefCatSurg FRANZCO is an ophthalmologist specialising in refractive, cataract, and corneal surgery. She is Co-Founder and Director of Eagle Eye Surgeons, a boutique practice in two Sydney locations.
Dr Erica Darian-Smith MBBS MMed GradDipRefCatSurg FRANZCO is an ophthalmologist specialising in refractive, cataract, and corneal surgery. She is Co-Founder and Director of Eagle Eye Surgeons, a boutique practice in two Sydney locations.
Trained at Prince of Wales Hospital in Sydney, she completed a two-year fellowship in corneal and refractive surgery and external eye diseases in Toronto, Canada. There, she gained subspeciality expertise in refractive surgery and treatment of all corneal diseases, including corneal transplants. Dr Darian-Smith is a fellow of the World College of Refractive Surgery and Visual Sciences and serves as a Visiting Medical Officer at Nepean Public Hospital in Sydney.

Dr Margaret Lam
Dr Margaret Lam BOptom is Head of Optometry Services at 1001 Optometry in Bondi Junction and an Adjunct Senior Lecturer at the University of New South Wales’ School of Optometry and Vision Science. She practises full-scope optometry with a focus on myopia management, dry eye, and specialty contact lenses, including orthokeratology and keratoconus. She is a past National President of Optometry Australia.
References
- Tear Film and Ocular Surface Society, Dry eye redefined, TFOS DEWS II report, available at tfosdewsreport.org [accessed Sept 2025].
- Mikalauskiene L, Grzybowski A, Zemaitiene R. Ocular surface changes associated with ophthalmic surgery. J Clin Med. 2021 Apr 12 10(8):1642. doi: 10.3390/jcm10081642.
- Stapleton F, Alves M, Jones L, et al. TFOS DEWS II Epidemiology report. Ocul Surf. 2017 Jul;15(3):334-365. doi: 10.1016/j.jtos.2017.05.003.
- Stapleton F, Argüeso P, Dogru M, et al. TFOS DEWS III: Digest. Am J Ophthalmol. 2025 Jun 4;279:451-553. doi: 10.1016/j.ajo.2025.05.040. Epub ahead of print.
- Gomes JAP, Azar DT, Wolffsohn JS, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017 Jul;15(3):511-538. doi: 10.1016/j.jtos.2017.05.004.
- Gupta PK, Drinkwater OJ, Starr CE, et al. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg 2018;44:1090-6. doi: 10.1016/j.jcrs.2018.06.026.
- Trattler WB, Majmudar PA, Goldberg D, et al. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017; Aug 7;11:1423-1430. doi: 10.2147/OPTH.S120159.
- Cochener B, Cassan A, Omiel L. Prevalence of meibomian gland dysfunction at the time of cataract surgery. J Cataract Refract Surg. 2018;44:144–8. doi: 10.1016/j.jcrs.2017.10.050.
- Albietz JM, Lenton LM, McLennan SM. The effect of ocular surface management on myopic LASIK outcomes. Cornea. 2000;19(6):S73.
- Corbett MC, O’Brart DPS, Warburton FG, Marshall J. biologic and environmental risk factors for regression after photorefractive keratectomy. Ophthalmology 1996;103:1381–91. doi: 10.1016/s0161-6420(96)30494-6.
- Albietz JM, Lenton LM, McLennan SG, McLennan SG. Chronic dry eye and regression after laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2004;30:675-84. doi: 10.1016/j.jcrs.2003.07.003.
- Oh T, Jung Y, Kim H, et al. Changes in the tear film and ocular surface after cataract surgery. Jpn J Ophthalmol. 2012;56(2):113-118. doi: 10.1007/s10384-012-0117-8.
- Australian Institute of Health and Welfare (AIHW), What procedures were performed, In: Admitted patient care 2018–19: Australian hospital statistics. AIHW; 2019.
- Australian Commission on Safety and Quality in Health Care. New standard to improve care for Australians with cataract (media release, 17 Aug 2021) Available at: safetyandquality.gov.au/newsroom/media-releases/new-standard-improve-care-australians-cataract [accessed Sept 2025].
- Haman Optical Maryborough. LASIK & Refractive Surgery Co-Management [Internet]. Maryborough (QLD): Haman Optical Maryborough. Available at: hamanopticalmaryborough.com.au/eye-care-services/lasik-refractive-surgery-co-management/ [accessed Sept 2025].
- Eye Laser Specialists. Is laser eye surgery worth it? [Internet]. Australia: Eye Laser Specialists. Available at: eyelaserspecialists.com.au/is-laser-eye-surgery-worth-it/ [accessed Sept 2025].
- Epitropoulos, AT. Treating DED in refractive cataract patients. Ophthalmic Management. 2020;24:18-20.
- Szakáts I, Sebestyén M, Tóth É, Purebl G. Dry eye symptoms, patient-reported visual functioning, and health anxiety influencing patient satisfaction after cataract surgery. Curr Eye Res. 2017;42(6):832–836. doi: 10.1080/02713683.2016.1262429.
- Kawahara A. Management of dry eye disease for intraocular lens power calculation in cataract surgery: a systematic review. Bioengineering (Basel). 2024 Jun 11;11(6):597. doi: 10.3390/bioengineering11060597.
- Epitropoulos AT, Matossian C, Berdy J, Malhotra RP. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672-1677. doi: 10.1016/j.jcrs.2015.01.016.
- Koh S, et al. Effect of unstable tear film and optical quality after cataract surgery. Am J Ophthalmol. 2017;180:18-24.
- Yeh TN. Ocular surface disease: Impact on pre-surgical biometry and symptoms in refractive and cataract surgery. Alcon Medical Affairs White Paper. 2023. Available at: alcon.widen.net/view/pdf/qod1d9tecs/CA_Ocular-surface-disease–impact-on-pre-surgical-biometry-and-symptoms_WP_p-MED-CA-ILU-250001.pdf [accessed Sept 2025].
- Benítez-del-Castillo J, Labetoulle M, Boboridis K, et al. Visual acuity and quality of life in dry eye disease: Proceedings of the OCEAN group meeting. Ocul Surf. 2017 Apr;15(2):169-178. doi: 10.1016/j.jtos.2016.11.003.
- Wolffsohn JS, Benítez-Del-Castillo JM, Jones L, et al; + TFOS collaborator group. TFOS DEWS III: Diagnostic Methodology. Am J Ophthalmol. 2025 May 30;279:387-450. doi: 10.1016/j.ajo.2025.05.033. Epub ahead of print.
- Jones L, Downie LE, Craig JP, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017 Jul;15(3):575-628. doi: 10.1016/j.jtos.2017.05.006.
- Jones L, Craig JP, Wolffsohn JS, et al; + TFOS Collaborator Group. TFOS DEWS III: Management and Therapy. Am J Ophthalmol. 2025 Jun 2;279:289-386. doi: 10.1016/j.ajo.2025.05.039. Epub ahead of print.
- Lyseng-Williamson KA. Cationorm (cationic emulsion eye drops) in dry eye disease: a guide to its use. Drugs Ther Perspect. 2016; 32:317-322. doi: 10.1007/s40267-016-0319-0.
- Daull P, Amrane M, Garrigue JS, et al. Cationic emulsion-based artificial tears as a mimic of functional healthy tear film for restoration of ocular surface homeostasis in dry eye disease. J Ocul Pharmacol Ther. 2020 Jul/Aug;36(6):355-365. doi: 10.1089/jop.2020.0011.
- Cationorm package information.
- Optometry Australia. Optometry Connection Dry Eye Resource Guide 2024:24-31.
- Amrane M, Creuzot-Garcher C, Baudouin C, et al. Ocular tolerability and efficacy of a cationic emulsion in patients with mild to moderate dry eye disease – a randomised comparative study. J Fr Ophtalmol. 2014 Oct;37(8):589-98. doi: 10.1016/j.jfo.2014.05.001.
- Aragona P, Spinella R, Rania L, Postorino E. Assessment of the efficacy of Cationorm® in patients with moderate dry eye compared with Optive® and Emustil® eye drops. Acta Ophthalmologica. 2011;89(Suppl s248). doi: 10.1111/j.1755-3768.2011.3125.x.
- Robert PY, Cochener B, Baudouin C, et al. Efficacy and safety of a cationic emulsion in the treatment of moderate to severe dry eye disease: a randomized controlled study. Eur J Ophthalmol. 2016 Nov 4;26(6):546-555. doi: 10.5301/ejo.5000830.
- Memona MAS, Ibraheem HD, Rizwan B, et al. Pak J Heal Sci 2022; 3(4):32-36. doi: 10.54393/pjhs.v3i04.86.
- Jaworski D, Cieślińska-Rypolc A, Kałużny BJ, et al. Cationic nanoemulsion vs. 0.15% sodium hyaluronate artificial tears in the healing process following modern surface keratorefractive surgery. Eur J Ophthalmol. 2023 Nov;33(6):2178-2184. doi: 10.1177/11206721231169540.