

Vision has an important role in driving, with vision impairment resulting from eye diseases having a negative impact on driving outcomes, including performance and safety. In this review, Professor Joanne Wood and Associate Professor Alex Black discuss the impact of glaucoma, one of the most common causes of irreversible vision impairment, on these driving outcomes. They explore studies that report driving performance and safety outcomes in drivers with glaucoma, compared to age-similar control groups of drivers with normal vision, as well as studies that have explored how the extent of glaucomatous visual field loss impacts on driving. Finally, they discuss the implications of these findings for driver licensing.
Self-Reported Driving Difficulties
Drivers with glaucoma report high levels of difficulty with driving and avoidance of challenging driving situations, including driving at night and in rainy conditions.1-7 Glaucoma is also linked to driving cessation, with those drivers with more extensive glaucomatous field loss being more likely to cease driving.3,4,6
Off-Road Hazard Perception Tests
In general older driver studies, delays in response times using off-road computer-based hazard perception tests (HPT) have been associated with poorer on-road performance, higher rates of heavy braking events, and increased crash risk.8-12 Studies show delays in HPT response times in drivers with glaucoma compared to controls, with delays of 0.42s (n=30)13 and 1.19s (n=20).14 Greater field loss in the worse eye was associated with more delayed HPT response times,13 and more extensive scanning in those with glaucoma was associated with faster (better) hazard response times,13,15 suggesting that adoption of compensatory behaviours may improve performance.
Driving Simulator Performance
Studies of driving simulator performance of drivers with glaucoma, compared to controls, showed mixed findings based on various outcome measures. In one study, drivers with glaucoma (n=23) exhibited more jerky steering and poorer target detection than controls, but no other differences.16 In a case-control study, patients with advanced glaucoma (n=43) had significantly more simulator collisions than controls, which were associated with reduced binocular integrated visual field sensitivity.17 In more recent studies, drivers with moderate to severe glaucomatous defects (n=14) exhibited longer reaction times to hazards (pedestrians and oncoming vehicles) and poorer lane keeping compared to controls,18 with another study reporting poorer vehicle control (steering and lane keeping) in drivers with glaucoma (n=25) compared to controls.19 The potential for compensatory scanning was also demonstrated in a small study of drivers with glaucoma (n=6) compared to controls, where drivers with glaucomatous field loss who passed a driving simulator test (n=3) demonstrated increased scanning eye and head movements.20
Closed and On Road Driving Performance
One study of closed road driving performance demonstrated poorer overall driving scores and more hazards hit by drivers with glaucoma (n=13) compared to controls.21
In this study, larger saccadic eye movements in those with glaucoma were associated with better driving performance, suggesting compensatory behaviours.21
Several studies have also demonstrated that drivers with glaucoma have poorer on-road driving performance, including overall performance,22-24 and more instructor interventions,23,25,26 than controls. In particular, drivers with glaucoma demonstrated problems with lane keeping, negotiating curves, and anticipatory skills,22,23 which were exacerbated in complex driving situations, such as at traffic lights and intersections.23 Drivers with glaucoma also received increased numbers of driving instructor interventions (braking or steering wheel) than controls,23,25,26 or were rated as less safe than controls.24 However, one study found similar driving performance between drivers with glaucoma and controls.27 These studies have a number of limitations, including small numbers of drivers with glaucoma, typically around 20 or less with a range of field loss.24-27 Only Wood, Black and colleagues23 have assessed larger numbers of drivers with glaucoma (n=75).
The evidence regarding the association between the severity of field loss and on-road driving performance is mixed. More restricted kinetic visual fields were associated with poorer lane keeping and anticipatory skills,22 and the mean deviation index in the worse eye was associated with an overall rating of driving and instructor interventions in another study.26 However, other studies have failed to find associations between severity of visual field loss and unsafe driving performance.25,27 Indeed, another study showed that the extent of scanning eye movements rather than field loss was related to driver safety ratings.24 While the number of participants in this study was relatively small (n=10), this study does highlight the potential for compensation for field loss through eye or head movements.
Self-Reported and State-Recorded Crashes
Studies of crashes have reported mixed evidence regarding glaucoma and crash risk, based on either self-reported or state-recorded motor vehicle crashes (MVCs).
In some studies, the rate of self-reported MVCs in the past five years for drivers with glaucoma (n=17 and n=25) was similar to controls,27,28 while other studies showed higher rates for drivers with glaucoma (n=40 and n=48), compared to controls.29,30 However, these studies were limited by small sample sizes, and differences in the severity of glaucomatous visual field loss. A larger study of 121 drivers with glaucoma reported that the rate of self-reported MVCs in the past 10 years increased with greater severity of glaucoma.5 In their study, drivers with severe glaucoma (defined as mean deviation -10 dB or worse in the worse eye) were 10 times more likely to be involved in a self-reported MVC in the past 10 years compared with control drivers, yet the MVC rates were similar between drivers with mild or moderate glaucoma and controls. Studies using self-reported MVC outcomes are, however, limited by potential recall biases, such as inaccurate recall or misreporting of previous MVCs, and lack of detail on the severity of visual field loss at the time of the MVC.
There is also mixed evidence from studies using state or police-recorded MVC data. In earlier studies, the rates of state-recorded MVCs in the past five years of drivers with glaucoma (n= 48 and n= 43) were either similar to controls,30,31 or higher for drivers with glaucoma (n=19) compared to controls.32 In a large study, 576 drivers with glaucoma were less likely to be involved in a state-recorded MVC in the previous five years than controls, and there were no differences in the rates of at-fault crashes and controls.1 In a more recent study of 206 drivers with glaucoma,33 the state-recorded at-fault MVC rate among drivers with glaucoma was 1.6 times higher than controls.
There is good evidence that greater severity of visual field loss is associated with higher state-recorded MVC risk in drivers with glaucoma. In a study of 240 drivers with glaucoma, those with moderate or severe visual field impairment (24-2 fields) in the worse eye were over three times more likely to be involved in a state-recorded at-fault MVC in the past five years, compared to those with no defect.34 In a study of 206 drivers with glaucoma using a novel visual field test, those with severe visual field loss were over two times more likely to be involved in a state-recorded at-fault MVC in the past five years compared to those with less-severe visual field loss, while MVC rates were not associated with impaired visual acuity or contrast sensitivity.33 Similarly, in a study of 438 drivers with glaucoma, those with severely impaired pattern deviation indices in their binocular fields were over two times more likely to be involved in a state-recorded MVC in the past five years, compared with those who were not severely impaired.35
Recommendations For Driver Licensing
Glaucoma is a progressive eye disease that can cause visual field impairment, so a perimetry-based assessment of visual fields is required in addition to assessment of visual acuity. The 2022 Assessment of Fitness to Drive (AFTD) guidelines36 indicate that a binocular Esterman is required for a patient with any monocular visual field defects or a progressive eye condition. As such, all patients with glaucoma should complete a binocular Esterman test to confirm if the standard is met. Fixation monitoring must be performed and recorded, and the test is only considered reliable if the false-positive score is no more than 20%.
If an Esterman test shows any missed points, then the clinician is required to check for the presence of any missed points within the central 20° area from fixation (i.e. 40° area in diameter), in addition to the horizontal extent.
For the central 20° area from fixation, a patient with glaucoma does NOT meet the standard for an unconditional private licence in the presence of either:
- A cluster of four or more adjoining points that is either completely or partly within the central 20° area, or
- Loss consisting of both a single cluster of three adjoining missed points up to and including 20° from fixation, and any additional separate missed point(s) within the central 20° area.
For the horizontal extent, a glaucoma patient does not meet the standard for an unconditional licence if the binocular visual field does not have a horizontal extent of at least 110° within 10° above and below the horizontal midline. Conditional licences may be recommended by optometrists, provided the extent of the horizontal visual field is at least 90° or greater. However, further research is required to better understand the role of conditional licensing for drivers with glaucoma, in terms of balancing patient mobility and independence, and community road safety.
An example of the monocular and binocular field plots of a patient with glaucoma is shown in Figure 1, with the assessment of the central 20° and horizontal field extent criteria applied. While the AFTD guidelines indicate that other assessments, including contrast sensitivity and glare assessments, may be considered when assessing a patient with glaucoma, how clinicians incorporate these additional tests into fitness to drive recommendations remains unclear. The possibility that some drivers with glaucoma might be able to compensate for their field loss by increased scanning of the road environment has also been suggested from both closed and open road studies.20,21 This remains an unexplored area that requires further research.
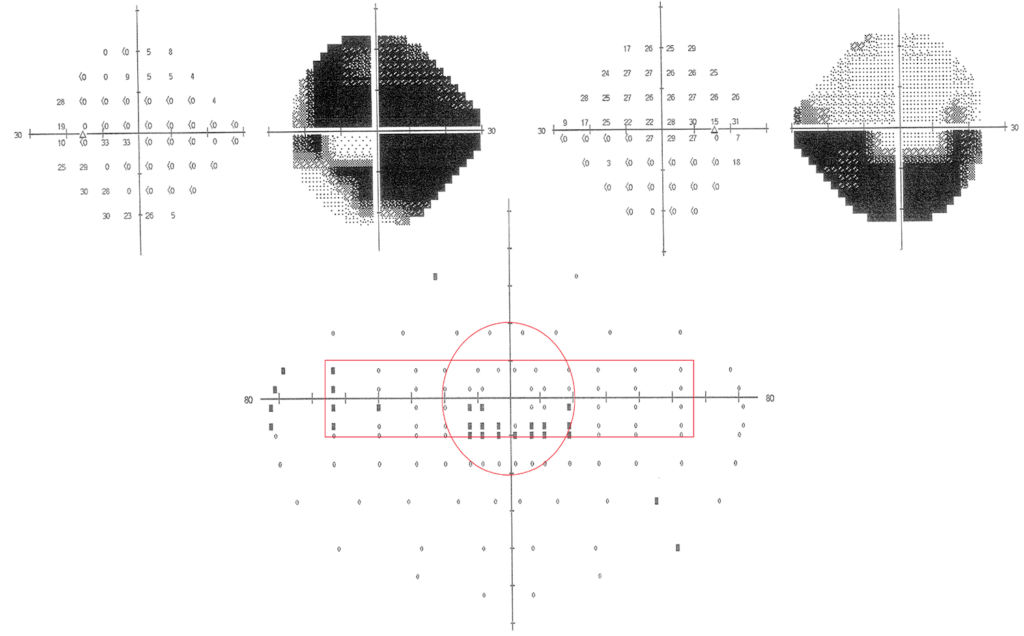
Figure 1. Example of a driver with glaucomatous field loss with the fitness to drive criteria applied.
In summary, there is evidence that some, but not all, drivers with glaucoma experience challenges with aspects of driving, as some studies suggest they are less safe when compared to age-similar controls, particularly in those with greater field loss. However, the extent of field loss associated with unsafe driving behaviours is challenging to define, as drivers may appropriately adopt restricted driving patterns and compensatory behaviours, such as increased caution and scanning of the road environment. In conclusion, the issue of glaucoma and driving is complex, given the multifactorial nature of driving, involving vision, physical capacity, cognition and insight. Thus, making decisions that balance a patient’s need for mobility and independence with driving safety remains challenging.
Joanne Wood PhD DSc (Hon) MCOptom FAAO FARVO is a Professor in Optometry and Vision Science, Faculty of Health, at Queensland University of Technology (QUT) and has extensive research experience in areas including: vision and driving, vision and falls, children’s functional vision, and clinical psychophysics. Her research experience spans more than 25 years, including a PhD in Visual Sciences at Aston University, UK, followed by a Post Doctoral Fellowship in Clinical Psychophysics at Oxford University. Prof Wood’s research has resulted in the publication of over 280 articles, and presentation of more than 200 research papers at major international conferences. She is a member of the Vision and Everyday Function research group, within the Centre for Vision and Eye Research.
Alex Black PhD MPH BAppSc (Optom) FAAO is an Associate Professor and Course Coordinator for the Master of Optometry (OP85) Program within Optometry and Vision Science, Faculty of Health, Queensland University of Technology. His research interests focus on vision, ageing, and visual impairment, and their impacts on functional everyday activities, such as mobility and driving. He is a member of the Vision and Everyday Function research group, within the Centre for Vision and Eye Research.
References
- McGwin G Jr, Mays A, Owsley C, et al. Is glaucoma associated with motor vehicle collision involvement and driving avoidance? Invest Ophthalmol Vis Sci. 2004 Nov;45(11):3934-9. doi: 10.1167/iovs.04-0524.
- Yamasaki T, Yuki K, Asaoka R, et al. Binocular superior visual field areas associated with driving self-regulation in patients with primary open-angle glaucoma. Br J Ophthalmol. 2021 Jan;105(1):135-140. doi: 10.1136/bjophthalmol-2019-315187.
- Ramulu PY, West SK, Friedman DS, et al. Driving cessation and driving limitation in glaucoma: the Salisbury Eye Evaluation Project. Ophthalmology. 2009 Oct;116(10):1846-53. doi: 10.1016/j.ophtha.2009.03.033.
- van Landingham SW, Hochberg C, Ramulu PY, et al. Driving patterns in older adults with glaucoma. BMC Ophthalmol. 2013 Feb 21;13:4. doi: 10.1186/1471-2415-13-4.
- Tanabe S, Yuki K, Tsubota K, et al. The association between primary open-angle glaucoma and motor vehicle collisions. Invest Ophthalmol Vis Sci. 2011 Jun 13;52(7):4177-81. doi: 10.1167/iovs.10-6264.
- Janz NK, Musch DC, Niziol LM, et al. Collaborative Initial Glaucoma Treatment Study (CIGTS) Investigators. Evaluating clinical change and visual function concerns in drivers and nondrivers with glaucoma. Invest Ophthalmol Vis Sci. 2009 Apr;50(4):1718-25. doi: 10.1167/iovs.08-2575.
- Freeman EE, Muñoz B, Friedman DS, et al. Glaucoma and quality of life: the Salisbury Eye Evaluation. Ophthalmology. 2008 Feb;115(2):233-8. doi: 10.1016/j.ophtha.2007.04.050.
- Wood JM, Horswill MS, Anstey KJ, et al. Evaluation of screening tests for predicting older driver performance and safety assessed by an on-road test. Accident Analysis & Prevention. 2013;50:1161-8. doi: 10.1016/j.aap.2012.09.009.
- Hill A, Horswill MS, Whiting J, Watson MO. Computer-based hazard perception test scores are associated with the frequency of heavy braking in everyday driving. Accident Analysis & Prevention. 2019;122:207-14. doi: 10.1016/j.aap.2018.08.030.
- McKenna FP, Horswill MS. Hazard perception and its relevance for driver licensing. Journal of the International Association of Traffic and Safety Sciences. 1999;23:26-41.
- Horswill MS, Hill A, Wetton M. Can a video-based hazard perception test used for driver licensing predict crash involvement? Accid Anal Prev. 2015 Sep;82:213-9. doi: 10.1016/j.aap.2015.05.019.
- Darby P, Murray W, Raeside R. Applying online fleet driver assessment to help identify, target and reduce occupational road safety risks. Safety Science. 2009;47:436-42. doi: 10.1016/j.ssci.2008.05.004.
- Lee SS, Black AA, Wood JM. Effect of glaucoma on eye movement patterns and laboratory-based hazard detection ability. PLoS One. 2017;12(6):e0178876. doi: 10.1371/journal.pone.0178876.
- Wood JM, Black AA, Anstey KJ, Horswill MS. Hazard perception in older drivers with eye disease. Transl Vis Sci Technol. 2021 Jan 22;10(1):31. doi: 10.1167/tvst.10.1.31.
- Crabb DP, Smith ND, Garway-Heath DF, et al. Exploring eye movements in patients with glaucoma when viewing a driving scene. PLoS One. 2010 Mar 16;5(3):e9710. doi: 10.1371/journal.pone.0009710.
- Prado Vega R, van Leeuwen PM, Rendón Vélez E, Lemij HG, de Winter JC. Obstacle avoidance, visual detection performance, and eye-scanning behavior of glaucoma patients in a driving simulator: a preliminary study. PLoS One. 2013 Oct 16;8(10):e77294. doi: 10.1371/journal.pone.0077294.
- Kunimatsu-Sanuki S, Iwase A, Fukuchi T, et al. The role of specific visual subfields in collisions with oncoming cars during simulated driving in patients with advanced glaucoma. British Journal of Ophthalmology. 2017;101(7):896-901. doi: 10.1136/bjophthalmol-2016-308754.
- Adrian J, Authié C, Gutman E, et al. Driving behaviour and visual compensation in glaucoma patients: Evaluation on a driving simulator. Clin Exp Ophthalmol. 2022;50(4):420-8. doi: 10.1111/ceo.14062.
- Anderson DE, Bader JP, Ndulue JK, et al. Glaucomatous visual fields and neurocognitive function are independently associated with poor lane maintenance during driving simulation. BMC Ophthalmol. 2020;20(1):419. doi: 10.1186/s12886-020-01682-9.
- Kübler TC, Kasneci E, Rosenstiel W, Heister M, Aehling K, Nagel K, et al. Driving with glaucoma: Task performance and gaze movements. Optometry & Vision Science. 2015;92(11):1037-46. doi: 10.1097/OPX.0000000000000702.
- Lee SS, Black AA, Wood JM. Scanning behavior and daytime driving performance of older adults with glaucoma. Journal of glaucoma. 2018;27(6):558-65. doi: 10.1097/IJG.0000000000000962.
- Bowers A, Peli E, Owsley C, et al. On-road driving with moderate visual field loss. Optom Vis Sci. 2005;82(8):657-67. doi: 10.1097/01.opx.0000175558.33268.b5.
- Wood JM, Black AA, Owsley C, et al. Glaucoma and driving: On-road driving characteristics. PLoS One. 2016;11(7):e0158318. doi: 10.1371/journal.pone.0158318.
- Kasneci E, Sippel K, Schiefer U, et al. Driving with binocular visual field loss? A study on a supervised on-road parcours with simultaneous eye and head tracking. PLoS One. 2014;9(2):e87470. doi: 10.1371/journal.pone.0087470.
- Bhorade AM, Yom VH, Carr D, et al. On-road driving performance of patients with bilateral moderate and advanced glaucoma. American Journal of Ophthalmology. 2016;166:43-51. doi: 10.1016/j.ajo.2016.02.031.
- Haymes SA, LeBlanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Glaucoma and on-road driving performance. Investigative Ophthalmology & Visual Science. 2008;49(7):3035-41. doi: 10.1167/iovs.07-1609.
- Devos H, Ranchet M, Akinwuntan AE, et al. Performance-based visual field testing for drivers with glaucoma: A pilot study. Traffic Inj Prev. 2018;19(7):715-21. doi: 10.1080/15389588.2018.1508834.
- Szlyk JP, Taglia DP, Paliga J, Deepak PE. Driving performance in patients with mild to moderate glaucomatous clinical vision changes. Journal of Rehabilitation Research and Development. 2002;39(4):467-82. PMID: 17638144.
- Szlyk JP, Mahler CL, Wilensky JT, et al. Driving performance of glaucoma patients correlates with peripheral visual field loss. Journal of glaucoma. 2005;14(2):145-50. doi: 10.1097/01.ijg.0000151686.89162.28.
- Haymes SA, Leblanc RP, Chauhan BC, et al. Risk of falls and motor vehicle collisions in glaucoma. Investigative Ophthalmology & Visual Science 2007;48:1149-55. doi: 10.1167/iovs.06-0886.
- McCloskey LW, Koepsell TD, Wolf ME, Buchner DM. Motor vehicle collision injuries and sensory impairments of older drivers. Age and Ageing 1994;23(4):267-73. doi: 10.1093/ageing/23.4.267.
- McGwin G, Jr., Owsley C, Ball K. Identifying crash involvement among older drivers: agreement between self-report and state records. Accident Analysis and Prevention 1998;30(6):781-91. doi: 10.1016/s0001-4575(98)00031-1.
- Kwon M, Huisingh C, Owsley C, et al. Association between glaucoma and at-fault motor vehicle collision involvement among older drivers: A population-based study. Ophthalmology. 2016;123(1):109-16. doi: 10.1016/j.ophtha.2015.08.043.
- McGwin G Jr, Xie A, Owsley C, et al. Visual field defects and the risk of motor vehicle collisions among patients with glaucoma. Invest Ophthalmol Vis Sci. 2005 Dec;46(12):4437-41. doi: 10.1167/iovs.05-0750.
- McGwin G, Jr., Huisingh C, Jain SG, Girkin CA, Owsley C. Binocular visual field impairment in glaucoma and at-fault motor vehicle collisions. Journal of glaucoma. 2015;24(2):138-43. doi: 10.1097/IJG.0b013e3182a0761c.
- Assessing Fitness to Drive. 6th ed: Austroads Ltd; 2022. Available at austroads.gov.au/drivers-and-vehicles/assessing-fitness-to-drive [accessed Dec 2025].






