

Promising research shows Descemet’s stripping only / Descemetorhexis without endothelial keratoplasty can improve visual acuity in early to intermediate stage Fuchs’ endothelial corneal dystrophy, without corneal transplantation.
Corneal transplantation has been the only treatment for corneal endothelial failure for decades. We have always thought that the corneal endothelial monolayer is locked in the G1 phase of the cell cycle and unable to replicate in the event of cell loss. Recent studies have demonstrated that endothelial cell proliferation can occur, and can be expedited with Rho-associated protein kinase (ROCK) inhibition. ROCK inhibitors promote corneal endothelial cell proliferation, advancing cells past the G1 phase.
there have been increasing reports of spontaneous clearing of the cornea in the presence of DM trauma… or following prolonged detachment of the donor graft as a complication following EK surgery

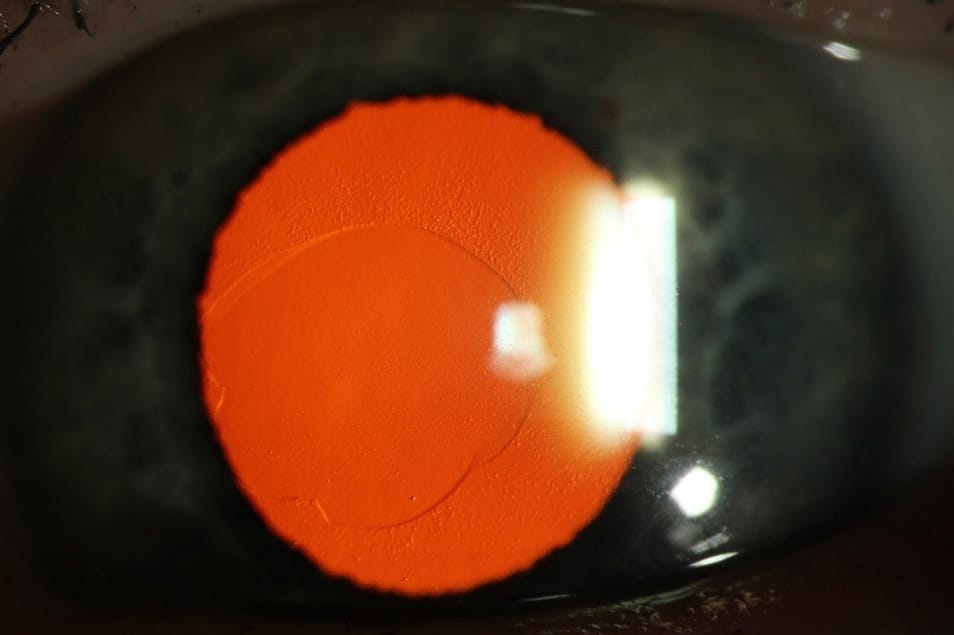
Figure 1. Retroillumination photo of descemetorhexis with corneal clearance.
In early to intermediate stage Fuchs’ endothelial corneal dystrophy (FED), Descemet’s stripping only / Descemetorhexis without Endothelial Keratoplasty (DSO/DWEK) has been shown to improve visual acuity without the need for corneal transplantation. The benefits of a clear cornea without the inherent risks associated with transplantation are certainly an exciting prospect for patients.
This potential intermediary step is now available before offering corneal transplantation in a clinical trial setting. Refinement in its technique and further prospective studies are required to establish its role in the management of FED. We are currently recruiting for the trial at the Royal Victorian Eye and Ear Hospital (RVEEH): DWEK trial with and without concurrent use of ROCK inhibitors (email: elaine.chong@eyeandear.org.au).
FUCHS’ ENDOTHELIAL DYSTROPHY
The cornea consists of five layers:
- The outermost epithelium,
- Bowman’s layer,
- Stroma,
- Descemet’s membrane (DM), and
- The innermost endothelium.
The endothelium consists of a single layer of endothelial cells which pump fluid away from the cornea to help maintain its transparency. A reduction in endothelial cell density and function can occur as the result of intraocular surgery, trauma and corneal dystrophies including FED. In FED, the loss of endothelial cells around corneal guttata, which are small excrescences of the DM, results in vision degradation and can cause glare and halos. FED is currently the most common cause of corneal endothelial cell failure, which in late stages, leads to corneal oedema and loss of vision.
THE ESTABLISHED TREATMENT
In the past, corneal failure was traditionally managed with a full thickness corneal transplant known as penetrating keratoplasty, where all five layers of the cornea were replaced with donor cornea tissue. Over the last 10 years, the surgical technique for transplantation has changed dramatically, with endothelial keratoplasty (EK) becoming the procedure of choice for isolated endothelial disease. The principle of EK is to remove only the affected layers, namely the endothelium and the overlying Descemet’s membrane (DM), in a procedure called a ‘descemetorhexis’, and to replace them with the equivalent layers from a donor cornea tissue. This means the overlying clear host stroma is not disturbed or transplanted, with only a small incision required to insert the transplant into the anterior chamber. The transplant is then attached to the posterior cornea with the help of air tamponade, along with face up positioning which requires patient cooperation. This minimally invasive surgery has resulted in faster visual recovery and better tectonic strength.
There are two types of EK currently performed:
- A thicker EK, usually between 50μmto 150μm thick (requiring a 5mm cornealincision for insertion) comprising of DM with endothelial cells along with a thin layer of corneal stroma, known as ultrathin (if it is below 100μm thick) Descemet’s stripping automated endothelial keratoplasty (DSAEK), or
- A very thin EK comprising of onlyDM with its single layer of endothelialcells, a 10-20μm thin tissue (inserted via a smaller 2.75mm corneal incision), known as Descemet’s membrane endothelial keratoplasty (DMEK).
DSAEK is an established technique where DM, along with a layer of stroma, is transplanted with good results. DSAEK is a thicker graft but it is easier to handle surgically. DMEK surgery has a steeper learning curve but with refinement in its technique over the last few years, the visual outcomes for DMEK have been shown to be better than DSAEK.1
WHY DO WE NEED A NEW TREATMENT?
The endothelium was traditionally thought to ‘heal’ by a compensatory migration and hypertrophy of existing cells. The endothelium was considered a nonregenerating monolayer,2 due to an arrest of the endothelial cell cycle in the G1 phase, due to contact inhibition.3
ROCK inhibitors have been shown to improve cell adhesion and proliferation in the corneal endothelium
In recent years, there have been increasing reports of spontaneous clearing of the cornea in the presence of DM trauma (e.g. accidental DM removal at the time of cataract surgery or during other intraocular surgery), or following prolonged detachment of the donor graft as a complication following EK surgery, without the need for replacement corneal tissue.4-6
This triggered the question, how did the cornea clear without its DM along with its endothelial cells? Some postulate that a population of endothelial stem cells reside in the corneal periphery and maintain some regenerative function in adult life.7 Hence replication and migration can lead to repopulation of the areas of damage with resultant corneal clearance.
This postulation led to studies evaluating the possibility of removing a section of DM along with its diseased endothelial cells, without implanting an EK corneal graft, and simply leaving the cornea to heal on its own, for visual rehabilitation in Fuchs’ Endothelial Dystrophy (FED).8 This procedure is known as DWEK/DSO.9 Like any surgical technique, DWEK/DSO has evolved with time and experience. In recent cases, only a small section of diseased DM, along with its endothelial cells in the visual axis in early to intermediate FED, were removed and left to spontaneously heal. In these studies, the central guttata were visually significant and these were cases where DMEK corneal transplant would ordinarily be offered to the patient. These recent studies showed corneal clearance rates of between 63% to 100%.10-16
The thought of visual rehabilitation and improvement without the need for a corneal transplant is an attractive option for the patient. There are no innate risks associated with corneal transplantation – such as longterm steroid drops, steroid response with high increased intraocular pressure (IOP) before and graft rejection, graft failure, graft detachment, or incorrect graft orientation – because corneal transplant is not required and not performed. Similarly, mandatory 48 hour face-up positioning after DMEK transplant surgery is not required.
WHERE IS DWEK/DSO IN THE TREATMENT ALGORITHM?
DWEK can be thought of as the potential intermediate step between observation and DMEK corneal transplantation. If DWEK surgery fails, where the patient’s own peripheral endothelial cells are unable to repopulate the central cornea resulting in persistent corneal oedema, DMEK corneal transplant can still be performed without issues.
Potential treatment algorithm for Fuchs’ Endothelial Dystrophy:
- Conservative treatment / observation(if asymptomatic),
- DWEK/DSO (if symptomatic,potential new treatment),
- DMEK corneal transplant(if DWEK/DSO fails).
Early studies of DWEK involved very large areas of DM removal – between 6mm to 8mm in diameter – and corneal clearance rates were low.17,18 Refined surgical techniques, enabling delicate DM removal without deep scoring and indentation of the posterior stroma during removal, as well as removal of only a 4mm diameter of DM, led to improved corneal clearance rates. Four out of five consecutive cases10 and 10 out of 13 retrospective cases with a 4mm descemetorhexis (DM scoring) achieved corneal clearance,11 while nine out of 12 prospective cases with a 4mm descemetorhexis achieved corneal clearance.12 Even though there was an improvement in the rates of corneal clearance with a smaller descemetorhexis, questions remain unanswered. Why are there non-responders and slow-responders? What patient, surgical and environmental factors encourage DWEK success?
WHO IS SUITABLE FOR DWEK/DSO?
Careful patient selection is important. Adequate and sufficient healthy peripheral endothelial cells are required to ensure sufficient reserve cells that can migrate and replicate into the gap created by the descemetorhexis. Peripheral cell count of more than 1,000 cells/mm2 on confocal microscopy is an inclusion criterion for DWEK/DSO. Persons with advanced corneal stroma oedema with extensive haze and bullae are not suitable. A history of herpes simplex keratitis or cytomegalovirus keratitis, or secondary corneal pathologies are not suitable.
WHAT ARE ROCK INHIBITORS?
Rho kinase is a serine/threonine protein kinase. Activation of RhoA protein (a small GTPase) results in activation of Rho kinase which then phosphorylates various intracellular substrates, including the myosin light chain, and the LIM kinase. These downstream substrates then control actomyosin contractility, membrane permeability, cellular adhesion, cell morphological changes, extracellular matrix organisation, and DNA synthesis.25 Therefore, Rho kinase has an important role in regulating cell shape and size, adhesion, reorganisation, and apoptosis.26 Not surprisingly, Rho-associated protein kinase (ROCK) inhibition affects various ocular conditions, briefly discussed below.
- Research in Rho kinase began in the 1990s, with the majority focussed onthe effect on IOP lowering. ROCK inhibitors have been shown to alter cell shapein the trabecular meshwork, which improved aqueous humour outflow with resultant IOP lowering.25
- Diabetic retinopathy and macula oedema occur when fluid extrudes into themacula, resulting in vision loss. This is due to the hyperpermeability of retinalcapillaries, where there is increased leukocyte adhesion, leading to endothelial damage and hence fluid extrusion.27 ROCK pathways promote leukocyte adhesion to microvascular structures, through increased levels of activated Intercellular Adhesion Molecule-1 (ICAM-1) and expression of other downstream proteins. Treatment with ROCK inhibitors reduces adhesion of leukocytes to microvascular structures, decreasing diabetic retinopathy and resultant macular oedema.28
- ROCK inhibitors have been shown to improve cell adhesion and proliferationin the corneal endothelium.29 They improve corneal endothelial cell migrationand decrease cell apoptosis. Apart from their adjunctive use in DWEK/DSO, they are also used in corneal endothelial cell culture techniques to improve uptake and engraftment onto host tissue.
Cell Culture and ROCK Inhibitors
A 2018 study of 11 patients was published in the New England Journal of Medicine, evaluating the effects of corneal endothelial cell culture injected into the anterior chambers of the study eye together with ROCK inhibitors.30 This was an uncontrolled, single-arm study, where the corneal endothelium was mechanically removed in an area measuring approximately 8mm diameter, without removing Descemet’s membrane. Human corneal endothelial cells were grown and cultured from a donor cornea and injected with a ROCK inhibitor (300μl) into the anterior chamber of the eye. After the procedure, patients were placed in a prone position for three hours to enhance engraftment of cultured cells onto the recipient tissue. The primary outcome was restoration of corneal transparency with central corneal endothelial cell density > 500 cells/mm2 at 24 weeks. There was 100% success in corneal clearance (11 out of 11). Secondary outcomes were corneal thickness <630μm (10 out of 11) and improvement in best corrected visual acuity of more than or equal to two lines at 24 weeks (nine out of 11). This small study has huge implications on the trajectory of corneal transplant and treatment.
WHAT WE KNOW SO FAR
In vitro studies have shown better endothelial cell migration from younger patients and the presence of an intact DM helps cell migration,19 presumably as a result of a smooth surface to allow for cell sliding. This is consistent with the observation that surgical scoring of DM results in poorer outcomes, with fibrosis of the stroma and stromal nodules resulting in a poorer surface for cell sliding and migration.15 This can also result of increased astigmatism20 following DWEK/DSO. Davies showed an increased posterior float following DWEK, likely as a result in a decrease in corneal thickness in the central zone.20 If the small 4mm descemetorhexis is de-centred and partially off the visual axis, this can affect final visual outcome due to the change in posterior curvature. So far, most studies have been small and retrospective and have often combined DWEK/DSO with cataract surgery, which makes refractive assessment of the sole effect of DWEK difficult. Clearly, further studies to refine the technique are required.
A retrospective study compared 15 DMEK cases vs. 12 DWEK cases (combined with cataract surgery) and found post-operative pinhole visual acuity similar between the two groups; logMAR 0.16 +/- 0.09 vs logMAR 0.13 +/- 0.10 (P = 0.44). The average time to 20/40 vision for DMEK was 2.2 +/- 2.8 weeks compared with 7.1 +/- 2.7 weeks for DWEK (P, 0.01). However, they found more adverse events in their DMEK group8 with 53% of patients experiencing adverse events, including IOP (n = 7), anterior chamber inflammation (n = 1), and graft nonadherence (n = 1), with one patient requiring anterior chamber paracentesis (6.7%) and one patient (6.7%) requiring a re-bubbling procedure. Conversely, the DWEK group had no adverse events (P 0.01).14
We need more information on patient selection, factors influencing success rates, and decisions regarding commencement, dose and duration of ROCK inhibitor augmentation
Recent in vivo studies have confirmed and demonstrated that endothelial cell proliferation can occur, and have also shown that this can be expedited with ROCK inhibition.21,22 Downstream substrates from ROCK inhibition control actomyosin contractility, membrane permeability, cellular adhesion, cell stiffening, cell morphological changes, extracellular matrix organisation, as well as DNA synthesis.22 Ripasudil 0.4% (Glanatec; Kowa Company Ltd, Nagoya, Japan), a ROCK inhibitor eyedrop, was approved in Japan in 2014 to increase the outflow of the aqueous humour as a treatment for glaucoma and ocular hypertension.
Ripasudil resulted in cytoskeletal rearrangement (cell rounding and reduced actin bundles) and decreased cell junctional complex proteins in the trabecular meshwork and Schlemm’s canal endothelial cells, thus promoting aqueous outflow.23
The addition of Ripasudil eyedrops have been shown to salvage cases of DWEK/ DSO that were not clearing, with the planned DMEK transplantation cancelled after commencement of Ripasudil in two eyes that stalled at two to three months. In both cases, topical Ripasudil administered six times a day for two weeks resulted in complete corneal clearance.12
A recent prospective study of 18 DWEK/ DSO patients (performed with or without cataract surgery), where nine patients were put on Ripasudil 0.4% drops four times a day for two months immediately after surgery, and nine patients had no Ripasudil after DWEK, were followed up for 12 months after surgery. Persons in the Ripasudil observation group recovered vision more quickly (4.6 vs. 6.5 weeks, P 0.01). A 10% decrease in peripheral endothelial cell density was seen in the non Ripasudil observation group compared to pre-operative scans at the end of 12 months (P 0.05). Corneas of all 18 patients cleared. There were more adverse events in the Ripasudil arm, with one patient intolerant to topical Ripasudil drops because of constipation during use. One patient in the Ripasudil arm developed endothelial failure at one year post-op, and had DMEK transplantation.16
Side effects of ROCK inhibitors include conjunctival hyperaemia (>50%), ocular irritation, corneal verticillata, conjunctival haemorrhages and gastrointestinal side effects such as constipation.24
We need more information on patient selection, factors influencing success rates, and decisions regarding commencement, dose and duration of ROCK inhibitor augmentation. Prospective DWEK/ DSO studies are being performed in Australia, with collaborative studies at the Sydney Eye Hospital (study closed, principal investigator: Dr Gregory Moloney) and RVEEH (study is actively recruiting, principal investigators: Dr Elaine Chong and Dr Elsie Chan – email: elaine.chong@eyeandear.org.au). See Figure 1 for retroillumination photo of descemetorhexis in a study participant with corneal clearance.
Although the study is temporarily suspended due to the novel coronavirus disease pandemic, please continue to contact me with interested patients. Study participants will be contacted once normal clinic activities are resumed.
CASE STUDY
Mr Gregory* is an 83-year old gentleman who complained of difficulty seeing his golf ball during his weekly golf sessions. He had previous cataract surgery and intraocular lens implants many years ago with another surgeon, with visual acuity of 6/12 in his right eye and 6/15 in his left eye, best-corrected. He was unhappy with his vision and felt it could be improved. He did not report significant diurnal variation in his vision.
On examination, he had a very dense area of guttatta with pigmentation at the visual axis within a zone of 5mm. Pachymetry was 620 microns in his left eye. Posterior examination was within normal limits. We discussed surgical treatment for FED and he was initially keen to proceed with DMEK. However, his main apprehension was the need for face up positioning to ensure that the DMEK transplant attaches to the posterior aspect of his cornea. He lives alone and was worried that positioning for more than 24 hours without any external help was not feasible.
We then re-discussed the option of DWEK/ DSO clinical trial at the RVEEH. I sent him to the RVEEH where I reviewed him for further discussion. Mr Gregory then underwent various tests to ascertain that he was a suitable candidate for DWEK surgery. He needed to fulfil the strict inclusion criteria. Importantly, he had confocal microscopy to ensure that there were enough peripheral endothelial cells to allow for migration of the cells to the central defect following surgical descemetorhexis. He also understood the need for blood tests and very stringent follow up routines to ensure that we could monitor his progress. He was aware that if the procedure failed, he would proceed to DMEK transplant which would mean that he would need to position face up following surgery. He met with the whole team at RVEEH and Centre for Eye Research Australia.
After consideration, Mr Gregory decided to proceed with his left eye, 4mm Descemetorhexis only. DWEK/DSO was performed under sterile conditions in theatre and he was discharged with post-operative eye drops on the same day. As there was no corneal transplant, he did not need to adopt any face up positioning and he could proceed with his activities as normal. He understood that vision out of the operated eye would worsen initially while waiting for the endothelial cells to migrate centrally. He was monitored weekly for the first four weeks. His cornea was initially very oedematous as expected, but cleared up within the first four weeks without the need for Ripasudil rescue. Left visual acuity improved from 6/15 pre-operatively to 6/12 by month one, 6/7.5 by month two, and at 10 months post DWEK, visual acuity was 6/4.8 best corrected. There was good central re-population of endothelial cells demonstrated on follow up confocal microscopy. The study will have one year follow up data for all patients. This study also aims to evaluate Ripasudil use post DWEK.
CONCLUSION
Corneal transplantation surgery has evolved significantly over time. DWEK/ DSO is a very promising new surgical treatment for FED, with high success rates in selected cases. Further DWEK/ DSO studies surrounding patient selection, refinement of surgical techniques and refractive outcomes, as well as understanding the commencement, optimal dosage and duration of augmentation with ROCK inhibitors are required to refine the technique and to ensure patient safety. Clinical trials are underway and are recruiting at the RVEEH.
* Patient name changed for anonymity.
Dr Elaine Chong MBBS (Melb), MEpi, PhD, FAMS, FRANZCO is the head of ophthalmology at the Royal Melbourne Hospital, and is a consultant ophthalmologist in both the corneal and retinal units at the Royal Victorian Eye and Ear Hospital (RVEEH). Dr Chong is a dual fellowship trained ophthalmologist, who completed sub-specialty fellowship training in Medical Retina at the RVEEH, and Corneal, Cataract and Refractive Surgery at the Singapore National Eye Centre. Dr Chong was awarded the Gold Medal for Excellence at the RANZCO Advanced Clinical Exams in 2011 and has received various international awards for her work in corneal and retinal research. Dr Chong holds a PhD and Masters of Epidemiology from the University of Melbourne. She is a senior research fellow at the Centre for Eye Research Australia, section editor of the Clinical & Experimental Ophthalmology journal, and she sits in the RANZCO Victorian Branch committee and Australia New Zealand Cornea Society Executive committee. Dr Chong has her private rooms in Glen Iris (irissurgery.com.au), Doncaster and South East Melbourne.
To earn your CPD points from this article visit www. mieducation.com.au/dwek-a-new-treatment-forfuchs’- endothelial-dystrophy
References
1. Chamberlain W, Lin CC, Austin A, et al. Descemet Endothelial Thickness Comparison Trial: A Randomized Trial Comparing Ultrathin Descemet Stripping Automated Endothelial Keratoplasty with Descemet Membrane Endothelial Keratoplasty. Ophthalmology 2019;126(1):19-26.
- Joyce NC. Proliferative capacity of the corneal endothelium. Progress in Retinal and Eye Research 2003;22(3):359-89.
- Joyce NC. Proliferative capacity of corneal endothelial cells. Experimental eye research 2012;95(1):16-23.
- Balachandran C, Ham L, Verschoor CA, et al. Spontaneous corneal clearance despite graft detachment in descemet membrane endothelial keratoplasty. American Journal of Ophthalmology 2009;148(2):227-34.e1.
- Watson SL, Abiad G, Coroneo MT. Spontaneous resolution of corneal oedema following Descemet’s detachment. Clin Exp Ophthalmol 2006;34(8):797-9.
- Ziaei M, Barsam A, Mearza AA. Spontaneous corneal clearance despite graft removal in Descemet stripping endothelial keratoplasty in Fuchs endothelial dystrophy. Cornea 2013;32(7):e164-6.
- He Z, Campolmi N, Gain P, et al. Revisited microanatomy of the corneal endothelial periphery: new evidence for continuous centripetal migration of endothelial cells in humans. Stem Cells (Dayton, Ohio) 2012;30(11):2523-34.
- Moloney G, Chan UT, Hamilton A, et al. Descemetorhexis for Fuchs’ dystrophy. Canadian Journal of Ophthalmology Journal Canadien D’ophtalmologie 2015;50(1):68-72.
- Kaufman AR, Nose RM, Pineda R, 2nd. Descemetorhexis Without Endothelial Keratoplasty (DWEK): Proposal for Nomenclature Standardization. Cornea 2018;37(4):e20-e1.
- Iovieno A, Neri A, Soldani AM, et al. Descemetorhexis Without Graft Placement for the Treatment of Fuchs Endothelial Dystrophy: Preliminary Results and Review of the Literature. Cornea 2017;36(6):637-41.
- Borkar DS, Veldman P, Colby KA. Treatment of Fuchs Endothelial Dystrophy by Descemet Stripping Without Endothelial Keratoplasty. Cornea 2016;35(10):1267-73.
- Moloney G, Petsoglou C, Ball M, et al. Descemetorhexis Without Grafting for Fuchs Endothelial Dystrophy- Supplementation With Topical Ripasudil. Cornea 2017;36(6):642-8.
- Malyugin BE, Izmaylova SB, Malyutina EA, et al. [Clinical and functional results of one-step phaco surgery and central descemetorhexis for cataract and Fuchs primary endothelial corneal dystrophy]. Vestnik Oftalmologii 2017;133(6):16-22.
- Huang MJ, Kane S, Dhaliwal DK. Descemetorhexis Without Endothelial Keratoplasty Versus DMEK for Treatment of Fuchs Endothelial Corneal Dystrophy. Cornea 2018;37(12):1479-83.
- Davies E, Jurkunas U, Pineda R, 2nd. Predictive Factors for Corneal Clearance After Descemetorhexis Without Endothelial Keratoplasty. Cornea 2018;37(2):137-40. 16. Macsai MS, Shiloach M. Use of Topical Rho Kinase Inhibitors in the Treatment of Fuchs Dystrophy After Descemet Stripping Only. Cornea 2019;38(5):529-34.
- Koenig SB. Planned Descemetorhexis Without Endothelial Keratoplasty in Eyes With Fuchs Corneal Endothelial Dystrophy. Cornea 2015;34(9):1149-51.
- Arbelaez JG, Price MO, Price FW, Jr. Long-term follow-up and complications of stripping descemet membrane without placement of graft in eyes with Fuchs endothelial dystrophy. Cornea 2014;33(12):1295-9.
- Soh YQ, Peh G, George BL, et al. Predicative Factors for Corneal Endothelial Cell Migration. Investigative Ophthalmology & Visual Science 2016;57(2):338-48.
- Davies E, Pineda R, 2nd. Corneal Tomography Changes and Refractive Outcomes After Descemet Stripping Without Endothelial Keratoplasty. Cornea 2019;38(7):817-9.
- Okumura N, Koizumi N, Ueno M, et al. ROCK inhibitor converts corneal endothelial cells into a phenotype capable of regenerating in vivo endothelial tissue. Am J Pathol 2012;181(1):268-77.
- Okumura N, Kinoshita S, Koizumi N. Application of Rho Kinase Inhibitors for the Treatment of Corneal Endothelial Diseases. Journal of Ophthalmology 2017;2017:2646904.
- Garnock-Jones KP. Ripasudil: first global approval. Drugs 2014;74(18):2211-5.
- Moshirfar M, Parker L, Birdsong OC, et al. Use of Rho kinase Inhibitors in Ophthalmology: A Review of the Literature. Med Hypothesis Discov Innov Ophthalmol 2018;7(3):101-11.
- Rao PV, Pattabiraman PP, Kopczynski C. Role of the Rho GTPase/Rho kinase signaling pathway in pathogenesis and treatment of glaucoma: Bench to bedside research. Experimental Eye Research 2017;158:23-32.
- Hall A. Rho GTPases and the actin cytoskeleton. Science 1998;279(5350):509-14.
- Arita R, Hata Y, Nakao S, et al. Rho kinase inhibition by fasudil ameliorates diabetes-induced microvascular damage. Diabetes 2009;58(1):215-26.
- Ahmadieh H, Nourinia R, Hafezi-Moghadam A, et al. Intravitreal injection of a Rho-kinase inhibitor (fasudil) combined with bevacizumab versus bevacizumab monotherapy for diabetic macular oedema: a pilot randomised clinical trial. The British Journal of Ophthalmology 2019;103(7):922-7.
- Okumura N, Okazaki Y, Inoue R, et al. Effect of the Rho- Associated Kinase Inhibitor Eye Drop (Ripasudil) on Corneal Endothelial Wound Healing. Investigative Ophthalmology & Visual Science 2016;57(3):1284-92.
- Kinoshita S, Koizumi N, Ueno M, et al. Injection of Cultured Cells with a ROCK Inhibitor for Bullous Keratopathy. The New England Journal of Medicine 2018;378(11):995-1003.





