

Myopia is a global problem that requires a concerted, collaborative effort by all eye health professionals to ensure patients receive, and adhere to, the most appropriate treatment.
The rising prevalence and the risks of sight-threatening ocular pathology associated with myopia are well documented.1,2 By 2050, it is predicted that half of the world’s population (five billion people) will be myopic, with nearly one billion at a high risk of sight threatening ocular pathology.1
Since the coronavirus pandemic was first reported in December 2019… many young adults and children have spent increased time on electronics and restricted time outdoors
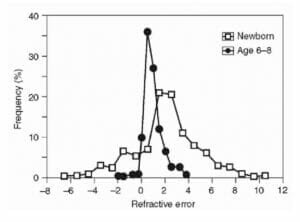
Figure 1. Refractive error at birth.14
Since the coronavirus pandemic was first reported in December 2019, and with subsequent unprecedented restrictions applied to the movement of more than three billion people (over a third of the world population), many young adults and children have spent increased time on electronics and restricted time outdoors.
This is the first time that over three billion people have been simultaneously exposed to the influence of cumulative, well-proven, risk factors for myopia. These excessive near-work activities may represent a greater risk of myopia for those with accommodative dysfunctions.
Given this milieu, there is a genuine and tenacious need to understand the pathogenesis of myopia, and to develop innovative solutions to ameliorate its effect on the population and on the economy.
WHAT IS MYOPIA?
While the exact etiology of myopia remains elusive, a long-running debate about whether myopia is predominantly genetic or environmental continues.3-5 The rising prevalence of myopia over recent decades has led to recognition that environmental effects must play an important role. Yet there remains strong evidence that genetic factors also make a significant contribution.

Figure 2. Four distributions of refraction, from two different studies from three months of age to 3.5 years; (A) three to nine months, Mutti et al and (B) one to three years, Ingram and Barr.13
Genetics
The first clear evidence for a genetic role in myopia came from twin studies, which showed identical (monozygotic) twins had a higher similarity (concordance) in refractive error than non-identical (dizygotic) twins.3 Such studies have estimated heritability for myopia to be as high as 91%. Associations between parent refraction and that of their children, have also been observed, indicating a potential genetic contribution.
Genome-wide association studies (GWAS) have identified >20 associated loci for myopia,4 but to date the causative genes have mostly proved elusive.5

Figure 3. Histograms of the distribution of refraction in
11–13-year-olds in Australia, Northern Ireland, and Japan.13
Interestingly, it appears genes that cause syndromic myopia contribute to myopia in the general population.6 Gene-based analyses have implicated 21 novel candidate myopia genes (ADAMTS18, ADAMTS2, ADAMTSL4, AGK, ALDH18A1, ASXL1, COL4A1, COL9A2, ERBB3, FBN1, GJA1, GNPTG, IFIH1, KIF11, LTBP2, OCA2, POLR3B, POMT1, PTPN11, TFAP2A, ZNF469). Furthermore, the development of myopia has been shown to be linked to different novel biological pathways; mannosylation, glycosylation, lens development, gliogenesis, and Schwann cell differentiation. This is different to hyperopia, which is mainly linked to organogenesis.6
It is important to understand the genetics of myopia, as this will ultimately discern the molecular signalling cascade and open up new avenues for intervention.
Environment
There is now consistent evidence that environmental factors play a role in the development of myopia – for instance, children who spend more time outdoors are less likely to be, or become, myopic.7-8 In western countries, we know that about two hours per day outdoors, out of school hours, eliminates the additional risk associated with more near-work as well as the risk associated with having myopic parents.
As health professionals, we need to work together to raise public awareness of myopia, its progression and complications
Increased time outdoors is effective in preventing the onset of myopia as well as in slowing the myopic shift in refractive error. But paradoxically, outdoor time is not effective in slowing progression in eyes that are already myopic. Further studies evaluating the effect of being outdoors in various doses, along with objective measurements of time outdoors, may help improve our understanding of the role outdoor time plays on onset and management of myopia.
The relationship between education and the high epidemic of myopia is strong and consistent, as described in 2018 by Morgan et al. It shows up in the association between myopia and years of schooling in adults, and during development in the associations between prevalence of myopia, accelerated learning streams and academic grades.9 In almost all studies which have addressed the issue, across a range of ethnic backgrounds, more educated people have been found to be more myopic.
Parental history of myopia is an important predictor in univariate and multivariate models, however the risk of myopia has been found to be further differentiated by the number of myopic parents and the hours in which a child participates in sports and outdoor activity. Children with two myopic parents and less participation in sports and outdoor activity were at increased risk of becoming myopic compared to children with either zero or one myopic parent. Children with no myopic parents who spent the most time engaged in sport and outdoor activities were the least likely to become myopic.
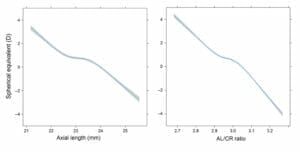
Figure 4. Association between spherical equivalent (in dioptres) and axial length in millimetres (left) and AL/corneal radius of curvature ratio (right) at nine years of age. The mean and 95% CI were adjusted for age, gender and height.16
TRIGGERS FOR MYOPIA
Before we proceed with myopia control, we need to understand some basic facts that stimulate eye growth and myopia development.
Thirty years ago, Phillips wrote that “the retina may not be the passive victim of scleral growth, but may conceivably be the author of its own destruction”.10 The retina has a central role in optically regulating eye growth and each area of the retina processes the retinal image and influences the growth and/or biomechanics of the overlying sclera. The existence of such mechanisms points to a highly complex interaction between the optics of the eye, the shape of the posterior segment, and the physiological mechanisms responsible for eye growth.11
The association of axial length (AXL) and peripheral refractive error in children prior to the onset of myopia is well known and has been extensively researched. Hyperopic defocus develops in the periphery of the eye along the horizontal meridian for a few years before the onset of myopia. Children who have a tendency to become myopic later, tend to become less hyperopic and have longer AXL. Compared to emmetropic children, they have more hyperopic relative peripheral refractive error, as calculated by the spherical equivalent (SE) of the average refraction in primary gaze subtracted from the SE of the average refractive error in 30° temporal gaze. This relative hyperopia is believed to be a growth signal due to a high lag of accommodation during near-work.12
One of the important predictive factors for myopia is a changing refraction. This arises from two apparently conflicting tendencies. First, the existence of a mechanism to control eye growth during infancy so as to bring refraction towards emmetropia/ low hyperopia (i.e. emmetropisation) and second, the tendency of many human populations to develop myopia during later childhood and into adulthood.
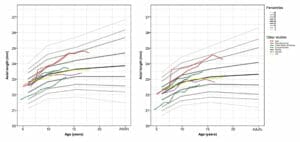
Figure 5. Axial length is plotted against age for male (left) and female (right) children from various geographic locations.16
To understand this, we need to elaborate more on human emmetropisation. It is important to appreciate that emmetropisation is only one of many homeostatic or disruptive processes affecting eye growth from conception to adulthood.13
By the age of six, the two principal determinants of refraction are the refraction at birth and the degree of emmetropisation that has occurred in the intervening years.
The presence of a significant refractive error at age six requires one of the following scenarios to apply: an initial refractive error too great to be corrected by emmetropisation; an initial refraction within the normal range but deficient emmetropisation; or a combination of both of these.
Large congenital refractive errors do exist but are rare, and are often associated with genetic disorders. Examples of clearly genetic congenital refractive errors include the congenital and non-progressive myopia associated with Stickler’s syndrome and Leber’s amaurosis. In such cases there appears to be a strong genetic bias away from emmetropia, and the large initial refractive errors remain largely unmodified by any emmetropisation mechanism. It is obvious that hyperopia and myopia behave differently, with most hyperopia arising from the persistence of infantile hyperopia due a failure of emmetropisation. The low incidence of myopia at age six, compared to older ages, indicates that the vast majority of myopia develops in eyes that have successfully emmetropised earlier in life. Myopia is therefore most commonly due to a secondary failure of the emmetropisation mechanisms to maintain emmetropia/low hyperopia.13
AXIAL LENGTH AND MYOPIA
In most cases, the refractive status of a newborn is hyperopia (Figure 1).14 In this instance, the retinal photoreceptors are in front of the focal plane. As the optics of the eye mature (the cornea flattens, anterior chamber deepens, and lens power decreases) the focal plane moves away from the cornea and ‘catches up’ with the retina, reaching emmetropia by the age of six to eight years. This process is guided by genetic factors as well as others (Figures 2 and 3).
AXL seems to be the most influential factor in emmetropisation of SE refractive error, while the cornea and crystalline lens lose substantial amounts of dioptric power in this phase of growth.15
if the target is not achieved using one method of control, it is always wise to try another approach
High myopia, which is defined as a SE of 6D or worse, generally corresponds to AXL ≥26mm, which drastically increases the risk of severe complications later in life, including myopic maculopathy, retinal detachment and glaucoma. High myopia in adulthood usually has a myopia onset before the age of 10, which progresses during teenage years and into the early twenties.16
Recently, Tideman et al were able to generate a growth chart for AXL based on large epidemiological cohorts of European children and adults. AXL (mm), corneal radius of curvature (CR), AXL/ CR ratio (calculated by dividing AXL in millimetres by CR in millimetres) were significantly higher in myopic children at nine years of age. However, there was no significant change in CR from six to nine years of age (Figure 4).
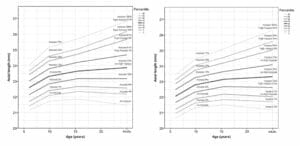
Figure 6. Growth chart depicting axial length in millimetres versus age for European study subjects, males (left) and females (right), with the risk of myopia in adulthood.
There is also a gender difference in AXL, CR and AXL/CR ratio, and racial difference; with the mean AXL value in Asian populations being larger after seven years of age than is the case in European populations17 (Figures 5 and 6).
Furthermore, AXL increases more rapidly in myopic children than in children with hyperopia.18 So, while there now appears to be some age-dependent normative data/percentile curves for AXL length,16,17,18 comprehensive percentile curves are not yet available.
MYOPIA MANAGEMENT
Prevention or control of myopia could be more effectively delivered using reliable predictive models for estimating the degree of risk. Ideally, predictive models achieve high sensitivity, so that all children who are likely to benefit from control of myopia are identified and can be offered appropriate interventions.
While a genetic test may be a useful addition to predictive tests, until a reliable test becomes available for clinical applications, a predictive model, which makes use of genetic indicators as well as a wide range of other information, appears likely to deliver the most clinically useful prognosis.
A prediction model for myopia can be achieved by obtaining the following patient information:
- History, including age, ethnicity, family history of myopia, and history of high myopia,
- Hobbies and outdoor activities,
- Refraction, compared to age, and
- AXL measurement.
There is a wealth of literature about myopia and different methods for its control – some of which work consistently well (e.g. orthokeratology (OK), dual focus contact lenses, and low dose atropine), and others which are not as effective, but may work.
Success can be monitored with AXL changes (≤0.2μm/ year for six to nineyear- old child). If the target is not achieved using one method of control, it is always wise to try another approach.
Recently there has been some controversy about the concentration of low dose atropine that can be used in myopia control. In 2006, the ATOM 1 (atropine for the treatment of childhood myopia) study, showed an 80% refractive and 100% AXL myopia controlling effect with 1% atropine compared to placebo. However, the significant side effects of mydriasis and cycloplegia made it less than tolerable as a first line treatment for progressive myopia.19
As health professionals, we need to work together to raise public awareness of myopia
ATOM 2 investigated 0.5%, 0.1% and 0.01% atropine for efficacy, and suggested that 0.01% is the optimal concentration with good efficacy and minimal side effects. Additionally, ATOM 2 found that in both refractive and AXL control, the results appeared to be more impressive with greater concentrations. Greater rebound effects were noted with the higher concentrations.20
Figure 7. Myopia awareness poster.
The Low-concentration Atropine for Myopia Progression (LAMP) study evaluated 0.05%, 0.025%, 0.01% atropine eye drops and a placebo group in 438 myopic children. The study firstly provided placebocompared evidence of low-concentration atropine eye drops in myopia control. Both efficacy and side effects followed a concentration-dependent response with 0.01% to 0.05% atropine. Among them, 0.05% atropine was the optimal concentration to achieve the best efficacy and safety profile. A recently published phase 2 report over two years, suggested the observed efficacy of 0.05% atropine was double that observed with 0.01% atropine, and it remained the optimal concentration among the studied atropine concentrations in slowing myopia progression.21
We are watching the horizon for randomised control trials, which will add, and consolidate, information we have on myopia control with low dose atropine. These may also help to answer unclear questions about low dose atropine in myopia control, and in particular, the efficacy of low dose (0.01%) atropine eye drops to reduce progression of myopia in children. Studies awaited include a multicentre placebo-controlled randomised trial in the UK (CHAMP-UK), the Myopia Outcome Study of Atropine in Children (MOSAIC), and the Western Australia Atropine for the Treatment of Myopia (WA-ATOM) study.22-24
Further studies are required to clarify other unclear aspects of atropine; including its formulation, mechanism of action, and stability.
OUR ROLE TO RAISE AWARENESS
As health professionals, we need to work together to raise public awareness of myopia, its progression and complications. The statistical results are alarming:
- In Australia and New Zealand, almost half (49% of Australian, and 46% of New Zealand parents of children aged 17 years and under) admit they do not know what causes myopia,
- Only 12% of parents in Australia and 10% in New Zealand know of the lifestyle factors that have an impact on childhood myopia (low levels of outdoor activity, low levels of light exposure, prolonged near tasks such as reading and gaming on portable devices), and
- 31% of Australian and 28% of New Zealand kids (17 years and under) have never been to have an eye examination.
OUR ROLE IN EDUCATION
As health professionals, we need to discuss, formulate and implement an agreed management plan with both parent/carer and patient (child).
This process should include:
- Educating on the risks (lifestyle and family history) of myopia progression,
- Discussing the available myopia management options to mitigate AXL elongation,
- Providing verbal and written information describing the risks and benefits of treatment, duration of treatment, review frequency, when to cease treatment, rebound effects, etc.,
- Documenting a review/recall for patients with myopia that will enable you to measure progression (increase of AXL),
- Monitoring the impact of treatment,
- Recognising personal limitations for treatment compliance, and • Referring patients who are myopes and high myopes to a suitable practitioner/ specialist if the required myopia management services cannot be provided.
CONCLUSION
Myopia is a global health crisis and a huge burden on the economy, both locally and worldwide. Myopia can have a significant socio-economic impact on the individual and puts them at increased risk for myopic maculopathy, retinal detachment, cataracts, and glaucoma – even for low and moderate levels of disease. These risks increase further with higher levels of myopia.
Continued efforts to increase the size and scale of genetic projects will bring about knowledge that will improve the ability to identify children most at risk of developing myopia for early treatment intervention.
Preventive strategies during containment should include a focus on visual habits, particularly among children and young adults (Figure 7).
AXL may serve as a key instrument for monitoring eye growth in children. Paediatric ophthalmologists, optometrists and orthoptists can use AXL growth charts to determine whether a child’s AXL is above average for his/her age, and this information can be used to estimate the risk of developing high myopia.
Additionally, children with a rate of AXL growth higher than expected, based on their percentile line, can be identified relatively early which will enable them to benefit from the increasing number of therapeutic options for preventing myopia.
Let us work together to slow myopia.
To gain your CPD points from this article visit mieducation.com/working-together-toslow- myopia.
Dr Rasha Altaie Mb.Ch.B, FRCSI, MSC, FRANZCO is an ophthalmologist who specialises in cornea and anterior segment reconstruction, and paediatric ophthalmology. Based in Auckland, Dr Altaie is honorary senior lecturer at the department of ophthalmology, Auckland University.
Dr Altaie is founder of the Myopia working group Australia and NZ, and Myopia Action Group NZ. Her main areas of research and interest are cornea and anterior segment, paediatric anterior segment diseases, myopia in children, its progression, and methods to slow myopia progression.
References
- Wolffsohn JS, Calossi A, Cho P et al. Global trends in myopia management attitudes and strategies in clinical practice. Cont Lens Anterior Eye 2016; 39: 106–116.
- Holden BA, Jong M, Davis S, Wilson D, Fricke T .& Resnikoff S. Nearly 1 billion myopes at risk of myopiarelated sight-threatening conditions by 2050 – time to act now. Clin Exp Optom 2015; 98: 491–493.
- Dirani M, Chamberlain M, Shekar SN, Islam AF, Garoufalis P, Chen CY, Guymer RH, Baird PN. Heritability of refractive error and ocular biometrics: the Genes in Myopia (GEM) twin study. Invest Ophthalmol Vis Sci. 2006 Nov;47(11):4756-61.
- Morgan IG. The biological basis of myopic refractive error. Clin Exp Optom 2003;86:276–288.
- Young TL. Molecular genetics of human myopia: An update. Optom Vis Sci 2009;86:E8–E22.
- Flitcroft DI, Loughman J, Wildsoet CF, Williams C, Guggenheim JA; CREAM Consortium. Novel Myopia Genes and Pathways Identified From Syndromic Forms of Myopia. Invest Ophthalmol Vis Sci. 2018 Jan 1;59(1):338-348.
- Dirani M, Tong L, Gazzard G, Zhang X, Chia A, Young TL, Rose KA, Mitchell P, Saw SM. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol. 2009 Aug;93(8):997-1000.
- French AN, Morgan IG, Mitchell P, Rose KA. Risk factors for incident myopia in Australian schoolchildren: the Sydney adolescent vascular and eye study. Ophthalmology. 2013 Oct;120(10):2100-8
- Morgan IG, French AN, Ashby RS, Guo X, Ding X, He M, Rose KA. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018 Jan; 62:134-149.
- Phillips, C.I., 1990. Aetiology of myopia. Br. J. Ophthalmol. 74, 47e48
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012 Nov;31(6):622-60.
- Mutti, D.O., Hayes, J.R., Mitchell, G.L., Jones, L.A., Moeschberger, M.L., Cotter, S.A., Kleinstein, R.N., Manny, R.E., Twelker, J.D., Zadnik, K., 2007. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest. Ophthalmol. Vis. Sci. 48, 2510e2519
- Flitcroft DI. Emmetropisation and the aetiology of refractive errors. Eye (Lond). 2014 Feb;28(2):169-79.
- Wick B. On the aetiology of refractive error, part I. A conceptual model. J Optom Vis Dev. 2000;31(1):5-21 with permission from the College of Optometrists in Vision Development.)
- Mutti DO, Mitchell GL, Jones LA, Friedman NE, Frane SL, Lin WK, Moeschberger ML, Zadnik K. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Invest Ophthalmol Vis Sci. 2005 Sep;46(9):3074-80.
- Tideman JWL, Polling JR, Hofman A, Jaddoe VW, Mackenbach JP, Klaver CC. Environmental factors explain socioeconomic prevalence differences in myopia in 6-yearold children. Br J Ophthalmol. 2018 Feb;102(2):243-247.
- Tideman JWL, Polling JR, Vingerling JR, Jaddoe VWV, Williams C, Guggenheim JA, Klaver CCW. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018 May;96(3):301-309.
- Breslin KM, O’Donoghue L, Saunders KJ. A prospective study of spherical refractive error and ocular components among Northern Irish schoolchildren (the NICER study). Invest Ophthalmol Vis Sci. 2013 Jul 18;54(7):4843-50.
- Chua WH, Balakrishnan V, Chan YH, Tong L, Ling Y, Quah BL, Tan D. Atropine for the treatment of childhood myopia. Ophthalmology. 2006 Dec;113(12):2285-91.
- Chia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A, Tan D. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012 Feb;119(2):347-54.
- Yam JC, Li FF, Zhang X, Tang SM, Yip BHK, Kam KW, Ko ST, Young AL, Tham CC, Chen LJ, Pang CP. Two-Year Clinical Trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020 Jul;127(7):910-919.
- Azuara-Blanco A, Logan N, Strang N, Saunders K, Allen PM, Weir R, Doherty P, Adams C, Gardner E, Hogg R, McFarland M, Preston J, Verghis R, Loughman JJ, Flitcroft I, Mackey DA, Lee SS, Hammond C, Congdon N, Clarke M. Low-dose (0.01%) atropine eye-drops to reduce progression of myopia in children: a multicentre placebocontrolled randomised trial in the UK (CHAMP-UK)-study protocol. Br J Ophthalmol. 2020 Jul.
- McCrann S, Flitcroft I, Strang NC, Saunders KJ, Logan NS, Lee SS, Mackey DA, Butler JS, Loughman J. Myopia Outcome Study of Atropine in Children (MOSAIC): an investigator-led, double-masked, placebo-controlled, randomised clinical trial protocol. HRB Open Res. 2019 Jul 23;2:15.
- Lee SSY, Mackey DA, Lingham G, Crewe JM, Richards MD, Chen FK, Charng J, Ng F, Flitcroft I, Loughman JJ, Azuara-Blanco A, Logan NS, Hammond CJ, Chia A, Truong TT, Clark A. Western Australia Atropine for the Treatment of Myopia (WA-ATOM) study: Rationale, methodology and participant baseline characteristics. Clin Exp Ophthalmol. 2020 Jul;48(5):569-579.





