Over the past few years, throughout her clinics, Melbourne retinal specialist Dr Christolyn Raj has seen an undoubted increase in the number of patients presenting for cataract surgery with co-existing diabetic eye disease.
In this article, Dr Raj discusses a step-by-step, evidence-based pre-operative protocol that can help patients with diabetes obtain the best possible results from cataract surgery.
LEARNING OBJECTIVES
On completion of this CPD activity, participants should:
1. Appreciate the clinical assessments involved in evaluating visual impairment from cataract versus diabetic eye disease,
2. Understand the intricacies of performing a baseline retinal evaluation,
3. Recognise the utility of ancillary investigations when triaging for diabetic eye disease severity, and
4. Realise the importance of clear communication to alleviate anxiety.
It has been well established that both type 1 and type 2 diabetes mellitus are risk factors for the development of particular types of cataract, in particular posterior subcapsular and cortical lens opacities. This risk profile particularly includes patients who are of younger age, have had a longer duration of diabetes, insulin use in type 2 diabetes, fluctuating glycaemic control, and the presence of diabetic maculopathy.1
Recently, I have had colleagues reaching out to me to provide advice on this subgroup of patients prior to them having cataract surgery. So, what are the typical questions I get asked? From a clinician’s perspective, my peers simply want to ‘do no harm’, and so many of their concerns are focussed on risk assessment. These include the timing of surgery: When is ideal? Are there particular pre-operative treatments that they should consider? What is the actual risk of post-operative inflammation in this patient cohort?
Interestingly, the patient’s perspective is entirely different. Most patients with diabetes commonly ask about their suitability for a premium intraocular lens (IOL), whether cataract surgery will also ‘treat’ their diabetic eye disease, and what their long-term follow-up plan will involve.
In this article, I discuss the answers to all these queries in an attempt to establish a robust pre-operative protocol that can assist in improving the outcomes of cataract surgery in this unique, though ever-increasing, subgroup of patients.
There is sound evidence internationally to suggest that patients with diabetic eye disease may also enjoy excellent visual outcomes post-surgery, however, the consensus has been made that their journey is somewhat different from their non-diabetic counterparts.2,3
Understanding this can assist us in our stepwise management of these patients, from the consulting room to the operating theatre to long-term follow-up.
The Gift of Prospective Clinical Trials
Prospective clinical trials have been instrumental in providing ‘real-world results’ in defining visual outcomes in diabetic patients following cataract surgery. While often a challenge to perform due to requirements – such as needing a specific patient demographic, ethics approval, and painstaking data collation – they have provided us with some much-needed answers.
Squirrel et al. showed that uncomplicated cataract surgery did not cause acceleration of diabetic retinopathy postoperatively.4 Romero-Aroca et al. reported progression of diabetic retinopathy in patients with higher levels of HbA1c and longer duration of diabetes.5 The incidence of pseudophakic diabetic macular oedema (DMO), believed to be higher in diabetic patients, varied among prospective studies, and has been reported with a wide range from 0.2% to 20%, depending on the clinical definition used.6
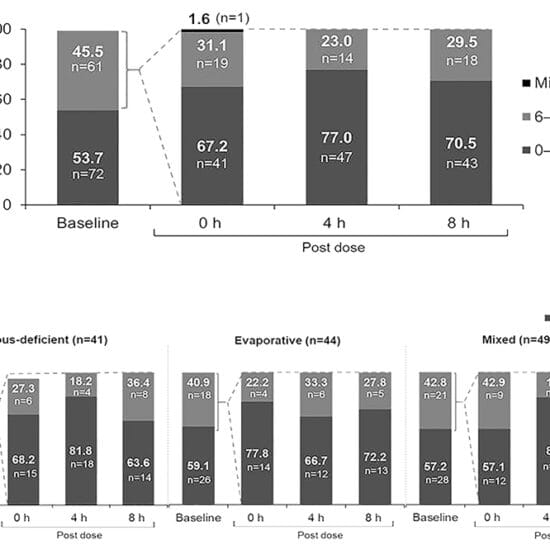
A recent multicentre prospective clinical study, conducted by my research group, looked at employing a standardised protocol in diabetic patients undergoing cataract surgery. Our study found that patients who are at particular risk of complications, in particular DMO, are those that have more significant retinopathy at baseline, as defined by the Diabetic Retinopathy Severity Score (DRSS) (R0.6, p<0.001), and those patients with prior treated maculopathy (R-0.46, p<0.002). The incidence of pseudophakic macular oedema in our study was 10.9% and found to be independent of retinopathy as per DRSS score (p = 0.06).7
Still further clinical trials are needed to look at other aspects of cataract surgery in diabetic patients. There are many unknowns, such as visual outcomes following use of extended depth of focus (EDOF) or multifocal IOLs.
When conducted, these clinical trials (like many) will have limitations in that some will involve smaller patient cohorts, some will be single-centre or single-surgeon studies, and will have differing follow-up periods.
The results of these types of trials, therefore, must be interpreted with some degree of caution. However, what they do offer us is undeniable evidence that a patient’s baseline diabetic eye disease can impact their outcome following cataract surgery, urging us to be thorough in our pre-operative assessment.
How Do We Prepare Patients for Cataract Surgery?
Our primary aim in any patient presenting for cataract surgery is to assess whether the visual changes are due to lens opacity versus other pathology. This is of paramount importance in patients with co-existing diabetic eye disease as there may be several causes of vision reduction.
A dilated fundus examination will assist here. It will firstly enable the complete visualisation of the lens, allow grading of the lens opacity, and confirm that this level of cataract correlates to the presenting visual acuity. It will also provide the means to grade the severity of diabetic retinopathy and maculopathy.
In our study, we used the DRSS, a standardised grading system, to define the stage of retinopathy. Essentially, this is a universally accepted classification where scores are assigned to the various stages of diabetic retinopathy. The DRSS ranges from level 10 (normal) to level 85 (advanced proliferative diabetic retinopathy (PDR)), as shown in summary format in Table 1.8,9

Table 1. The Diabetic Retinopathy Severity Scale.
Perhaps the most efficient way to screen patients using the DRSS is to take a colour fundus photo and assess each eye. It is helpful here to divide the retina into quadrants and assess each quadrant for microangiopathy from benign (microaneurysms and dot haemorrhages) to advanced (deeper retinal haemorrhage, hard exudates, cotton wool spots, and intraretinal microvascular abnormalities (IRMA)). The macula and paramacular region need to be assessed separately, focussing on the proximity of microaneurysms and/or hard exudates in relation to the fovea.
It has been reported that an increase in DRSS level from baseline is suggestive of an increased risk of developing vision-threatening PDR or DMO.
While this may seem academic, I can assure you it is not. This process can serve to completely alter the management course of the patient. For example, Figure 1 shows a patient with an early cataract with NPDR. When applying the DRSS, this would be classified as severe NPDR, prompting urgent referral and further investigation.

Figure 1. Patient with bilateral NPDR prior to laser treatment. A) right eye, B) left eye.

Figure 2. Fundus fluorescein angiogram of the same patient, showing areas of ischemia and neovascularisation.

Figure 3. The same patient with bilateral NPDR following panretinal photocoagulation.
A subsequent fundus fluorescein angiogram (FFA) showed areas of ischemia and neovascularisation (Figure 2). This patient required panretinal photocoagulation (PRP) and a period of careful follow-up for three months for insidious neovascularisation, prior to cataract surgery (Figure 3).
Is OCT Imaging Enough?
There is no question that optical coherence tomography (OCT) has revolutionised the way we manage our patients with diabetes. However, like any technology that offers us an instant ‘answer’, we must interpret what we are seeing with some clinical suspicion. Diabetic patients may still have maculopathy despite good vision and an absence of the classic features seen on OCT, namely intraretinal fluid cysts. We need to be wary of looking at other information that is provided in the OCT when interpreting whether maculopathy is present.
In our study, we found it useful to look at central macular thickness (CMT) pre- and post-operatively. There was a positive correlation between thickened pre-op CMT and ensuing development of pseudophakic macular oedema in some patients, perhaps suggesting the presence of sub-clinical maculopathy at baseline.
Another valuable sign to look for is the presence of hard exudate, seen as hyperreflective material in the inner retinal layers, suggestive of a previous leak from microaneurysms in the paramacular area. This should prompt a closer look at the region using a high magnification fundus lens, particularly looking for clusters of active microaneurysms which, if far away from the fovea, may be amenable to focal laser treatment.
An OCT-angiogram (OCT-A) can also be useful, particularly to identify macular ischemia. Much like in an FFA, this will often show an enlarged and irregular foveal avascular zone (FAZ). This is an important prognostic indicator for patients undergoing cataract surgery, as there may be limitations to the acuity that can be achieved, which needs to be discussed pre-operatively.10
How Can We Co-Manage These Patients?
Our role as eye care professionals is to advocate for and motivate our patients to optimise their diabetes, as we know this is likely to have positive impacts on their eye health in the long term. However, as in any chronic disease, it is often a challenge to ‘stay the course’. Patients will often find themselves in a harmful trajectory that they are unable to change by themselves. This is where we need to step in and form part of the multidisciplinary team.

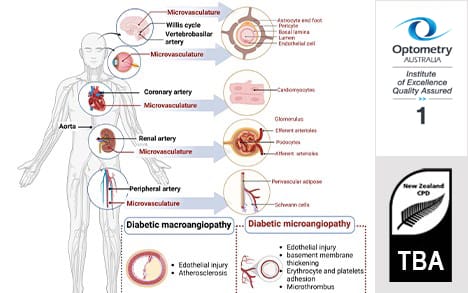
Figure 4. Micro- and macro-vascular complications of diabetes mellitus.13
I often spend time initially with patients highlighting how diabetes has the potential to affect every organ in the body, thus forming the basis of both microvascular (retinopathy, nephropathy, neuropathy) and macrovascular (cardiovascular, cerebrovascular, peripheral vascular disease) complications (Figure 4).
Because of these complications, we need to be in regular communication with the patient’s endocrinologist and general practitioner (GP) to coordinate our management. In some situations, there may be extraneous factors that need to be referred for appropriate management, such as smoking cessation, renal pathology, cardiovascular health, and mental health issues. Having a supportive team of specialists demonstrates to patients that ‘stability’ in their diabetes is holistic rather than a mere measurement of glycaemic status, as many have been accustomed to believing.
That is not to make light of the fact that optimal overall glycaemic control – as represented by the glycosylated haemoglobin level ( HbA1c) – is not important. Several studies to date have shown that patients who have a stable HbA1c and limited fluctuations in day-to-day blood sugar level (BSL) readings are less likely to have recurrence of retinopathy and/or maculopathy following cataract surgery.11,12 In my own clinics, I have found that patients who are able to measure their BSLs using a digital device (such as Dexcom, Freestyle libre) are at a slight advantage over their counterparts here, however this is not an affordable option for many patients.
What are the Long-Term Outcomes?
There is no reason that patients with diabetes can’t enjoy excellent visual outcomes following cataract surgery. This has been shown through several clinical studies to date.2 A key finding in almost all of these studies is the fact that their management course is inherently different to a patient without diabetes, and this needs to be discussed at the outset.
In some situations, patients may be appropriate for a particular type of IOL, others may not be good candidates. Depending on the stage of the diabetic eye disease, some patients may need to undergo a period of treatment prior to surgery involving intravitreal injections and/or laser. This may be followed by a period of careful observation prior to embarking on cataract surgery. All diabetic patients need to be co-managed effectively with their endocrinologist and GP, and it is often useful to have some gauge of their glycaemic status and control prior to surgery.
While this can seem a little daunting and unnecessary to a patient, explaining to them that taking these steps pre-operatively can make their recovery from surgery less complicated will often put patients at ease and motivate them to be invested in their outcomes.
References
- Wykoff C. Management of diabetes-related retinopathy. 2019 May. In: Prevention and Management of Diabetes-Related Eye Disease. Arlington (VA): American Diabetes Association; 2019 May. Available at: ncbi.nlm.nih.gov/books/NBK544520/. doi: 10.2337/db20191-11.
- Devgan U. Cataract surgery in diabetic patients: Excellent outcomes can be achieved in these patients with appropriate attention to details. Retina Today. 2010. Available at: retinatoday.com/articles/2010-july-aug/cataract-surgery-in-diabetic-patients [accessed May 2025].
- Chew E, Benson W, Ferris FL 3rd, et al. Results after lens extraction in patients with diabetic retinopathy: early treatment diabetic retinopathy study report number 25. Arch Ophthalmol. 1999;117:1600-1606. doi: 10.1001/archopht.117.12.1600.
- Squirrell D, Bhola R, Talbot JF, et al. A prospective, case controlled study of the natural history of diabetic retinopathy and maculopathy after uncomplicated phacoemulsification cataract surgery in patients with type 2 diabetes. Br J Ophthalmol. 2002;86(5):565-571. doi: 10.1136/bjo.86.5.565.
- Romero-Aroca P, Fernández-Ballart J, Buil-Calvo JA, et al. Non-proliferative diabetic retinopathy and macular edema progression after phacoemulsification: prospective study. J Cataract Refract Surg. 2006 Sep;32(9):1438-44. doi: 10.1016/j.jcrs.2006.03.039.
- Dowler J, Hykin PG. Cataract surgery in diabetes. Curr Opin Ophthalmol. 2001;12(3):175-178. doi: 10.1097/00055735-200106000-00005.
- Raj, C, Hodge C, Pathmaraj R, Bhatt U. Effectiveness of a standardised protocol in diabetic patients undergoing cataract surgery (in print).
- Staurenghi G, Feltgen N, Arnold J et al., VIVID-DME and VISTA-DME study investigators. Impact of baseline Diabetic Retinopathy Severity Scale scores on visual outcomes in the VIVID-DME and VISTA-DME studies. Br J Ophthalmol. 2018 Jul;102(7):954-958. doi: 10.1136/bjophthalmol-2017-310664.
- Koh A. Changing clinical paradigm in diabetic retinopathy. Retina Today: digital supplements. Available at: supplements.retinatoday.com/articles/ranibizumab-retinal-care-for-all-ages-rival-namd-to-rainbow-rop/changing-clinical-paradigm-in-diabetic-retinopathy. [accessed May 2025].
- Bromeo A, Grulla-Quilendrino P, Veloso A Jr, et al. Optical coherence tomography angiography analysis of changes in the foveal avascular zone in eyes with diabetic macular edema treated with intravitreal anti-vascular endothelial growth factor. Int J Retin Vitr. 2022 Aug 26;8(1):57. doi: 10.1186/s40942-022-00406-z.
- Wang, W, Fang, Y, Sun, Z. et al. Impact of HbA1c absolute change patterns on diabetic retinopathy risk in type 2 diabetes. Int J Diabetes Dev Ctries 2024. doi: 10.1007/s13410-024-01396-4.
- Zhao Y, Liu DC. Dynamic observation and analysis of factors influencing the progression of diabetic retinopathy. Exp Gerontol. 2024 Nov;197:112581. doi: 10.1016/j.exger.2024.112581.
- Li Y, Liu Y, Liu Y, et al. Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Signal Transduct Target Ther. 2023 Apr 10;8(1):152. doi: 10.1038/s41392-023-01400-z.