The management approach to diabetic retinopathy and diabetic macular oedema has evolved substantially in recent years, necessitating updates to clinical practice. This shift has been driven by two major factors: The rapidly increasing global prevalence of diabetes and the availability of newer, more effective ophthalmic treatments.
The International Diabetes Federation estimates that 589 million adults were living with diabetes in 2022, with this figure projected to reach 853 million by 2050.1 This growing disease burden demands scalable, effective, and evidence-based interventions from eye care providers.
Diabetes as a Systemic-Ocular Disease Continuum
Diabetic retinopathy (DR) must be understood within the broader context of diabetic microvascular and macrovascular disease. The pathophysiological mechanisms driving DR – including hyperglycaemia-induced oxidative stress, inflammatory cytokine production, retinal ischaemia, and VEGF upregulation – similarly affect renal, cardiovascular, and peripheral nervous systems.
Strong epidemiological associations exist between DR severity and diabetic nephropathy, with both conditions sharing common risk factors including poor glycaemic control, hypertension, and dyslipidaemia.2,3 Patients with proliferative diabetic retinopathy (PDR) demonstrate significantly higher rates of chronic kidney disease and cardiovascular events.4 This interconnection extends beyond mere statistical association: retinal vascular changes serve as a non-invasive window into systemic microvascular health, with DR severity potentially predicting cardiovascular and renal complications.
Optometrists play a pivotal role in the diabetes care continuum. Many patients present for routine eye examinations before developing symptomatic systemic complications, creating a valuable opportunity for early detection of DR and timely intervention. Identification of new-onset DR or evidence of progression, particularly in patients with suboptimal systemic control, should prompt communication with the patient’s general practitioner or endocrinologist. This facilitates optimisation of glycaemic control, blood pressure and lipid management, and consideration of referral for renal assessment where indicated.
In practice, comprehensive DR assessment should incorporate both structural and peripheral evaluation. Ultra-widefield (UWF) imaging allows detection of peripheral retinal lesions beyond standard photographic fields, which may influence grading and referral decisions. Optical coherence tomography (OCT) is essential for identifying diabetic macular oedema (DMO) and guiding urgency of referral. Together, these modalities support risk stratification and enable informed decisions regarding monitoring intervals and specific ocular treatment.

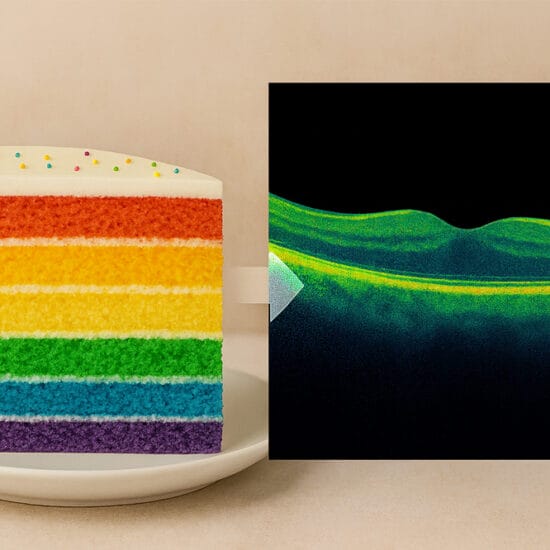
Figure 1A (top) Right eye OCT macula demonstrating DMO on presentation; VA 6/18 and Figure 1B (above) Right eye OCT four weeks after one intravitreal faricimab injection with resolution of DMO; VA 6/7.5.
Newer Systemic Diabetes Therapies and Retinal Implications
The introduction of glucagon-like peptide-1 (GLP-1) receptor agonists (eg., semaglutide, dulaglutide, and tirzepatide) has transformed the management of type 2 diabetes. These agents provide more effective glycaemic control than many traditional therapies and are associated with significant cardiovascular and renal benefits. Large cardiovascular outcome trials have established their role as preferred treatments in patients with diagnosed cardiovascular disease or high cardiovascular risk.5
However, the rapid reduction in HbA1c achievable with these effective agents has raised concerns regarding early worsening of diabetic retinopathy. This phenomenon, first described in the Diabetes Control and Complications Trial (DCCT), refers to a transient progression of retinopathy occurring within the first six to 12 months following intensification of glycaemic control.6 The proposed mechanism involves autoregulatory dysfunction: chronic hyperglycaemia induces compensatory retinal vasodilatation, and sudden normalisation of glucose levels causes relative ischaemia before microvascular remodelling can occur. This represents a physiological adaptation response to rapid glycaemia improvement rather than direct drug toxicity.
The SUSTAIN-6 trial of subcutaneous semaglutide reported increased rates of DR complications (including vitreous haemorrhage and the need for intravitreal therapy, or laser treatment) in the active treatment arm compared to placebo.7,8 Importantly, these events were predominantly observed early, in patients with pre-existing moderate to severe non-proliferative DR or PDR at baseline, and in those experiencing the most rapid HbA1c reductions.
Non-arteritic anterior ischaemic optic neuropathy (NAION) has emerged as a rare, but serious potential complication of GLP-1 receptor agonists, especially semaglutide. Observational cohort studies have suggested an increased risk, with a 2025 meta-analysis reporting a pooled hazard ratio of 2.6, with the risk becoming more apparent after two years of exposure.9 Regulatory bodies, including The European Medical Association and the World Health Organization, have recognised NAION as a very rare side effect of semaglutide, and issued safety communications.10 Eye care providers should consider baseline optic nerve assessment in high-risk patients – particularly those with a crowded optic disc, vascular risk factors, or prior fellow-eye NAION – prior to commencing semaglutide.
Practical monitoring recommendations for patients initiating GLP-1 receptor agonists include:
- Baseline comprehensive dilated fundus examination to establish DR severity and screening for a crowded disc or ‘disc at risk’,
- More frequent monitoring (every three to four months) for patients with moderate NPDR or worse during the first year of therapy,
- Clear communication with the patient’s GP or endocrinologist about baseline retinopathy status and recommended surveillance intervals,
- Maintain a low threshold for OCT imaging if clinical examination suggests macular oedema or unexplained visual change, and
- Patient education regarding symptoms of vitreous haemorrhage, tractional retinal detachment, or acute vision loss requiring urgent assessment.
It is crucial to emphasise that the long-term retinal benefits of improved glycaemic control far outweigh the risk of early worsening retinopathy. Eye care providers should support, rather than discourage, appropriate use of these agents while ensuring adequate surveillance.
Modern Diabetic Macular Oedema Management
Anti-VEGF therapy has become the undisputed first-line treatment for centre-involving diabetic macular oedema (CI-DMO). Randomised controlled trials, including DRCR.net Protocol T, have demonstrated superior visual outcomes with intravitreal anti-VEGF injections compared to focal/grid laser photocoagulation.11 Protocol T showed that in eyes with a baseline visual acuity worse than 6/15, aflibercept achieved superior visual gains, whereas outcomes were similar across aflibercept, bevacizumab, and ranibizumab with better baseline vision.
The introduction of faricimab (Vabysmo, Genentech), a bispecific antibody targeting both VEGF-A and angiopoietin-2 (Ang-2), represents an important advance in DMO management. The YOSEMITE and RHINE trials demonstrated non-inferior vision outcomes compared to aflibercept, with many patients achieving extended dosing intervals of 12–16 weeks following the loading phase.12 This improved durability addresses one of the major challenges in DMO management: treatment burden. Dual pathway inhibition may provide broader control of the complex pathophysiology underlying DMO, including vascular permeability and inflammation.
High-dose aflibercept 8 mg (Eylea 8 mg, Bayer) similarly offers extended dosing intervals of up to 20 weeks, with the PHOTON trial demonstrating non-inferiority to standard aflibercept 2 mg alongside meaningful reductions in treatment frequency.13,14 For eyes where anti-VEGF therapy is insufficient or not tolerated, intravitreal corticosteroids – such as triamcinolone acetonide or dexamethasone implant (Ozurdex) – provide an alternative, particularly in pseudophakic patients, by targeting the inflammatory component of DMO.
Real-world data generally support the efficacy of newer anti-VEGF agents, although outcomes are often modestly attenuated compared with clinical trial results due to less intensive monitoring and treatment schedules. The increasing use of treat-and-extend regimens, facilitated by longer-acting therapies, may improve patient adherence and reduce the socioeconomic burden of frequent visits, an important consideration, particularly for patients in rural or underserved areas.15

Figure 2. A) Left eye wide field fundus photograph demonstrating diabetic vitreous haemorrhage on presentation, with underlying tractional bands in a 24-year-old patient.

Figure 2B) Left eye four weeks after initial intravitreal ranibizumab injection, followed by panretinal photocoagulation, revealing tractional bands at the posterior pole and resolving vitreous haemorrhage inferiorly.
Laser Therapy in the Contemporary Era
While anti-VEGF therapy has become the first-line treatment for CI-DMO, laser photocoagulation continues to play a complementary role in diabetic eye disease management. Conventional focal or grid laser remains a reasonable option for non-centre-involving DMO, particularly in selected patients where access to intravitreal therapy is limited, there are contraindications to injections (e.g., pregnancy or recent cerebrovascular events), or where adherence to frequent treatment visits is a concern.
DRCR.net Protocol I established that all ranibizumab groups achieved superior visual outcomes compared to laser monotherapy. Importantly, deferring laser was at least as effective as prompt laser, with many patients in the deferred group never requiring laser treatment. These findings helped establish the contemporary paradigm of anti-VEGF first therapy, with laser reserved for refractory or non-centre-involving disease rather than used routinely at treatment initiation. Adjunctive laser may still have a role in reducing long-term injection burden in selected cases. However, conventional laser photocoagulation carries recognised risks, including permanent retinal scarring, that may enlarge over time and lead to scotomas or visual field loss. This has driven increasing interest in subthreshold laser techniques, which aim to minimise collateral retina damage while maintaining therapeutic benefit.16
Subthreshold micropulse laser (SML) has emerged as a promising alternative to conventional continuous-wave laser in the management of DMO. SML delivers laser energy in brief repetitive pulses with intervening rest periods, allowing thermal relaxation and minimising collateral damage to the retinal pigment epithelium and photoreceptors. Unlike conventional laser, SML produces no visible retinal laser burns, reducing the risk of scotoma formation, scar expansion, and other laser-related complications. The DIAMONDS trial provided high-quality comparative evidence that SML can achieve equivalent visual outcomes to conventional threshold laser over 24 months in eyes with DMO and central retinal thickness less than 400 μm.17 The critical advantage of SML lies in its favourable safety profile. The absence of visible retinal burns reduces the risk of inadvertent foveal injury and paracentral scotomas while preservation of photoreceptors and neurosensory retina allows treatment to be repeated without cumulative damage.
For ophthalmologists managing DMO in patients who do not meet Pharmaceutical Benefits Scheme (PBS) anti-VEGF criteria because of visual acuity restrictions, and where central macular thickness is <400 µm, DIAMONDS provides robust evidence that SML may be the preferred laser modality. It offers equivalent disease control with a superior safety profile, simplified delivery, and better overall value. The absence of visible burns makes SML particularly suitable for treatment close to the fovea and enables broader macular treatment without permanent retinal damage.
OCT has transformed laser treatment planning by enabling precise identification of macular thickening, intraretinal fluid, and microaneurysms. OCT-guided focal laser allows targeted treatment of leakage sources while avoiding areas of preserved retinal architecture, potentially improving both efficacy and safety. Similarly, OCT angiography (OCT-A) provides non-invasive visualisation of retinal perfusion abnormalities and may reduce reliance on fundus fluorescein angiography (FFA) in selected cases.
However, FFA retains an important role in the management of DR. Performing fluorescein angiography before commencing intravitreal therapy for DMO allows accurate assessment of retinal perfusion status, because retinopathy severity may appear to improve with anti-VEGF treatment, even when underlying perfusion deficits persist. Identifying patients at risk of neovascularisation before DMO resolves can help guide decisions about when to taper or cease anti-VEGF therapy. Although OCT-A is increasingly available, it still requires clear media and good patient cooperation, while widefield OCT-A remains limited in many clinical settings. The role of both modalities in guiding laser treatment continues to evolve.
Anti-VEGF vs Panretinal Photocoagulation in PDR
The management of PDR underwent a paradigm shift following publication of DRCR.net Protocol S, a landmark randomised trial comparing intravitreal ranibizumab with conventional panretinal photocoagulation (PRP).18 Protocol S followed patients with PDR for five years, with both treatments achieving excellent visual outcomes, maintaining average vision of 6/7.5 at five years. Protocol S demonstrated that ranibizumab was non-inferior to PRP for the primary outcome of visual acuity change at two years, with ranibizumab-treated eyes experiencing less peripheral visual field loss and fewer vitrectomy procedures.
However, the visual field advantage initially observed with ranibizumab diminished over time. Progressive peripheral field loss occurred beyond year two, such that by five years there was no significant difference in field loss between the two groups at five years. This attenuation is likely multifactorial, reflecting reduced treatment frequency over time as well as progression of the underlying DR. In patients without baseline centre-involved DMO, cost-effectiveness analysis demonstrated that ranibizumab alone is economically unfavourable compared to PRP.18,19
Anti-VEGF therapy offers several advantages in the management of proliferative diabetic retinopathy, including preservation of peripheral vision in the early phases, avoidance of laser-induced side effects, such as nyctalopia and reduced contrast sensitivity, and the ability to treat concurrent DMO with a single agent. However, these benefits must be weighed against important limitations. Anti-VEGF therapy requires frequent and often indefinite intravitreal injections (typically every four to eight weeks), resulting in substantial treatment burden and cost. There is also a small but real risk of injection-related complications, including endophthalmitis and retinal detachment, and a recognised risk of rapid disease reactivation if treatment is delayed or discontinued.
In contrast, PRP provides a more definitive treatment in most cases, with sustained regression of neovascularisation following a single treatment course. The ETDRS established that timely PRP reduces severe vision loss from PDR by more than 50%.20 Modern laser delivery systems, including pattern scanning lasers and navigated laser systems, have made PRP faster, more comfortable, and more precise than conventional techniques.
Hybrid treatment strategies, combining initial anti-VEGF therapy followed by deferred PRP, represent a pragmatic approach that captures benefits of both modalities. Ranibizumab became available on the PBS for proliferative diabetic retinopathy in 2025, formalising a combination approach that had previously relied on off-label anti-VEGF use. In contemporary practice, particularly in eyes with vitreous haemorrhage, combination therapy is often preferred: anti-VEGF is used to induce rapid regression of neovascularisation and facilitate clearance of haemorrhage, thereby creating a window for PRP, which provides more durable disease control, and reduces the risk of tractional retinal detachment and recurrent bleeding. Despite successful laser, reactivation of neovascularisation may still occur, occasionally necessitating further anti-VEGF therapy.
Treatment selection should be individualised, taking into account disease severity and the location of neovascularisation, the presence of DMO, the patient’s capacity to adhere to intensive injection regimens, geographic access to retinal services, occupational visual requirements, and out-of-pocket costs. In resource-limited settings, or in patients with unreliable follow-up, PRP remains an appropriate and often preferred monotherapy.
Vitreous Haemorrhage and the Shift Towards Earlier Surgery
Traditional management of diabetic vitreous haemorrhage has favoured initial observation or intravitreal anti-VEGF therapy, with vitrectomy reserved for cases that fail to clear spontaneously. However, DRCR.net Protocol AB has challenged this approach by directly comparing early surgical intervention with pharmacologic therapy. In this randomised trial, eyes with severe vision impairment due to vitreous haemorrhage were assigned to immediate vitrectomy or intravitreal aflibercept with deferred vitrectomy if required.21
The trial demonstrated that initial vitrectomy resulted in significantly faster visual recovery compared with intravitreal aflibercept alone. By six months, this difference had narrowed as some eyes in the aflibercept group underwent delayed vitrectomy or experienced spontaneous clearing of the haemorrhage. However, the early vitrectomy group maintained superior mean visual acuity. One-third of eyes (33%), initially randomised to the intravitreal aflibercept group, ultimately required vitrectomy over the two-year follow-up period. Importantly, initial vitrectomy reduced the rate of recurrent vitreous haemorrhage and enabled prompt identification and treatment of tractional retinal detachment, which may otherwise remain obscured by persistent haemorrhage.
The benefits of early vitrectomy extend beyond conventional visual acuity metrics to encompass broader quality-of-life outcomes. Prolonged periods of severe visual impairment due to vitreous haemorrhage can significantly affect independence, employment, driving ability, and psychological wellbeing. Rapid visual rehabilitation following early surgery may therefore address these important dimensions of patient welfare. However, these benefits must be balanced against the risks of surgery, postoperative recovery, and individual patient preferences.
Modern vitrectomy techniques utilising small-gauge instrumentation (25- or 27-gauge systems) have enabled sutureless surgery with faster recovery and reduced surgical morbidity compared to traditional 20-gauge approaches. Adjunctive pharmacotherapy with intravitreal anti-VEGF agents pre-operatively, or at the time of surgery, may reduce intraoperative bleeding and post-operative neovascular complications. However, the optimal timing remains an area of debate, balancing the benefits of neovascular regression against the potential risk of rapid fibrous contraction and progression of traction.
Individualised Approach: Putting it All Together
Contemporary management of diabetic eye disease has moved beyond rigid, algorithmic approaches towards personalised treatment strategies that integrate the best available evidence with patient-specific factors. This individualised paradigm recognises that similar degrees of DR or DMO may warrant different management decisions, depending on the broader clinical context.
Key disease-specific factors include the severity of DR, the presence and extent of macular oedema, prior treatment response, and the trajectory of systemic glycaemic control. Patient-related considerations include age, visual demands and occupational requirements, health literacy and the ability to recognise warning symptoms, reliability of follow-up, and socioeconomic factors such as access to transport, caregiver support, and financial resources, including insurance coverage.
Practical treatment paradigms illustrate how these principles translate into clinical decision making. In PDR complicated by vitreous haemorrhage, early vitrectomy with endolaser is often a preferred strategy, as it simultaneously clears media opacity, facilitates timely and complete panretinal photocoagulation under direct visualisation, and reduces the risk of tractional retinal detachment and recurrent haemorrhage.
For centre-involving DMO, intravitreal anti-VEGF therapy remains the standard first-line treatment, with agents such as aflibercept or ranibizumab widely used. Adjunctive SML may be considered to reduce long-term injection burden in selected cases. In eyes with visual acuity above PBS-eligibility thresholds, or where anti-VEGF therapy is contraindicated (e.g., pregnancy), SML represents a valuable alternative.
For non-centre-involved clinically significant DMO, focal/grid laser photocoagulation remains an appropriate first-line treatment. In pseudophakic patients with DMO refractory to anti-VEGF, intravitreal corticosteroids, such as triamcinolone acetonide or the dexamethasone intravitreal implant, provide an effective option by targeting the inflammatory component of macular oedema. Use of corticosteroids in phakic patients requires careful counselling regarding the risk of cataract progression.
Shared decision making represents best practice in this complex therapeutic landscape, with clinicians presenting evidence-based options while incorporating patient values and preferences. Patients should be supported to understand not only the anticipated benefits of different treatments, but also their associated burdens, risks, and alternatives. This collaborative approach enhances treatment adherence and patient satisfaction, while respecting individual autonomy.
Advances in imaging technologies, including ultra-widefield imaging, OCT, and OCT-A, have substantially enhanced assessment of diabetic eye disease. These modalities facilitate earlier detection of peripheral retinal pathology, quantitative monitoring of macular thickness, and identification of perfusion abnormalities without the need for pharmacological dilation or invasive angiography. However, such technologies complement, rather than replace, clinical judgement and clinicians must develop expertise in interpreting these findings within the broader clinical context.
Future Directions
Port Delivery System
The Port Delivery System (Susvimo, Genentech/Roche) represents an alternative treatment paradigm, comprising a surgically implanted, refillable reservoir providing continuous delivery of ranibizumab. This approach has the potential to substantially reduce treatment burden. While not currently approved by the Therapeutic Goods Administration, nor funded through the PBS in Australia, it has been approved by the Food and Drug Administration (FDA) in the United States since 2025.

Figure 3. A) External appearance of the port delivery system (PDS) after placement. B) Structure of the PDS.26
The Phase 3 PAGODA trial demonstrated that Susvimo, refilled every six months, achieved non-inferior visual acuity gains in patients with DMO compared with monthly ranibizumab injections (9.6 vs 9.4 letters).22,23 Two-year data confirmed sustained visual improvements and anatomical benefits, with 95% of patients not requiring supplemental ranibizumab injections.
For eyes with diabetic retinopathy without DMO, the Phase 3 PAVILION trial demonstrated 80.1% of patients receiving Susvimo, refilled every nine months, achieved at least a two-step DRSS improvement at one year, compared with only 9% in the control group, with no Susvimo patients requiring supplemental treatment.24 These results led to approval from the United States Food and Drug Administration in May 2025 for non-proliferative DR.25
Novel Therapeutic Targets
Novel therapeutic targets beyond VEGF pathway inhibition are under investigation. Interleukin-6 (IL-6) antagonists target the inflammatory component of DR and DMO, with early-phase studies demonstrating encouraging anatomical and functional outcomes.27
Tyrosine kinase inhibitors (TKIs) represent an emerging therapeutic class addressing anti-VEGF therapy’s primary limitation: treatment burden. Unlike biologic agents that inhibit VEGF extracellularly, TKIs act intracellularly to block multiple signalling pathways, including vascular endothelial growth factor receptor (VEGFR), platelet-derived growth factor receptor (PDGFR), fibroblast growth factor receptor (FGFR), and tyrosine kinase with immunoglobulin and epidermal growth factor homology domains 2 (Tie2), thereby providing broader pathway suppression. When combined with sustained-delivery platforms, these agents offer the potential for extended durability, with dosing intervals of up to six months. Several candidates show promise in diabetic eye disease. The Phase 3 VERONA trial of vorolanib (Duravyu intravitreal implant) demonstrated a mean visual acuity improvement of 7.1 letters, alongside an approximately two-thirds reduction in treatment burden at 24 weeks in patients with DMO.28 Similarly, axitinib-based formulations have shown promise, with extended dosing intervals approaching biannual administration. In the HELIOS trial, all treated eyes with non-centre-involving DMO demonstrated improvement at 48 weeks following a single injection.28,29 TKIs could fundamentally reshape DMO management through bi-annual treatments, improving real-world outcomes compared to monthly injection protocols currently required for anti-VEGF therapy.
Artificial Intelligence and Imaging Advancements
Artificial intelligence (AI) and machine learning are poised to transform DR screening and risk stratification. Automated DR grading algorithms have achieved sensitivity and specificity comparable to human graders in multiple validation studies, supporting their potential role in scalable screening programs, particularly in underserved populations.30 Beyond detection, AI-based predictive models integrating retinal imaging, OCT parameters, and clinical variables may enable identification of patients at high risk of disease progression, facilitating intensified surveillance and earlier, pre-emptive intervention.
OCT-A continues to evolve as a valuable adjunct in DR assessment. Quantitative OCT-A metrics, including capillary non-perfusion, foveal avascular zone enlargement, and characterisation of neovascular complexes, may offer non-invasive insights into retinal microvascular integrity and disease activity. As these technologies continue to advance – particularly with improvements in obtaining reliable outputs in the presence of media opacity – their clinical utility is likely to expand. These capabilities may reduce reliance on fluorescein angiography while providing novel biomarkers for monitoring disease progression and treatment response. However, broader integration of OCT-A into routine clinical practice will require standardisation of acquisition protocols, segmentation algorithms, and normative reference databases.
Conclusion
In 2026, management of diabetic retinopathy and macular oedema involves an expanding range of systemic therapies, advanced intravitreal agents, refined laser, and evolving surgical options. Effective care requires individualised, evidence-based planning that integrates disease severity, patient factors, and access to treatment, within a coordinated multidisciplinary framework that recognises diabetes as a systemic-ocular continuum. With the emergence of longer-acting therapies, novel pathway inhibitors, and AI-driven risk stratification, the potential to preserve vision has never been greater. Realising this potential, however, depends on prioritising early detection, optimising systemic disease control, and ensuring consistent longitudinal monitoring. Ultimately, the overarching goal remains the prevention of avoidable vision loss through timely intervention and coordinated, patient-centred care.
Key Take-Home Messages
- Diabetic retinopathy should be managed as part of a systemic disease continuum, requiring collaboration between eye care providers, endocrinologists, and GPs.
- Rapid improvement in glycaemic control may precipitate early worsening of DR through autoregulatory mechanisms. This has been observed with modern systemic therapies, including GLP-1 receptor agonists, and warrants closer retinal surveillance during the first year of treatment. Emerging data also suggest an association between GLP-1 receptor agonists and non-arteritic anterior ischemic optic neuropathy (NAION) in at-risk individuals.
- Anti-VEGF therapy remains first-line treatment for centre-involving DMO, with faricimab and high dose aflibercept 8 mg offering enhanced durability
- For patients with PDR without vitreous haemorrhage, DRCR.net Protocol S demonstrated non-inferiority of ranibizumab compared with laser PRP. However, laser PRP offers greater long-term durability. Initial treatment should therefore be individualised considering patient factors, access to care, follow-up reliability, and socioeconomic considerations. With the availability of ranibizumab on the PBS for PDR, many patients may be managed with initial anti-VEGF therapy to achieve rapid regression of neovascularisation, thereby creating a window for subsequent PRP to provide durable disease control.
- In diabetic vitreous haemorrhage, Protocol AB established benefits of early vitrectomy in selected cases, offering faster visual recovery and improved quality of life.
- Laser therapy retains an important role, with OCT-guided focal laser remaining first-line for non-centre-involved, clinically significant DMO, while subthreshold micropulse laser (SML) may be used as an adjunct to reduce anti-VEGF burden.
- Emerging therapies including longer-acting anti-VEGF agents, alternative pathway inhibitors such as IL-6 antagonists and TKIs, and AI-enabled screening have the potential to further improve outcomes and reduce treatment burden.
 Dr Jessica Xiong BMed/MD (UNSW) MMed (Ophth Sci) FRANZCO DRCPSC (Retina) is a medical retina specialist and vitreoretinal surgeon at Westmead, Concord, and Liverpool hospitals. She completed a medical retina fellowship at Westmead Hospital, a tertiary unit with a high-volume diabetic eye disease, and a vitreo-retina fellowship at the University of British Columbia, where she served as Chief Fellow. She is a Clinical Associate Lecturer with the University of Sydney and has contributed as a reviewer for Clinical and Experimental Ophthalmology.
Dr Jessica Xiong BMed/MD (UNSW) MMed (Ophth Sci) FRANZCO DRCPSC (Retina) is a medical retina specialist and vitreoretinal surgeon at Westmead, Concord, and Liverpool hospitals. She completed a medical retina fellowship at Westmead Hospital, a tertiary unit with a high-volume diabetic eye disease, and a vitreo-retina fellowship at the University of British Columbia, where she served as Chief Fellow. She is a Clinical Associate Lecturer with the University of Sydney and has contributed as a reviewer for Clinical and Experimental Ophthalmology.
 Professor Samantha Fraser-Bell BSc (Med) MB BS (Hons 1) MPH MHA PHD FRANZCO is a medical retina specialist and Professor of Ophthalmology at the University of Sydney. She is a consultant medical retina specialist at Royal North Shore and Sydney Eye Hospital. Her leadership roles include Co-Chair of the RANZCO Diabetic Retinopathy Screening Working Group, Deputy Director of Clinical Trials at the Save Sight Institute; Medical retina section editor for Clinical and Experimental Ophthalmology, and chair of the Australian Vision Research advisory committee.
Professor Samantha Fraser-Bell BSc (Med) MB BS (Hons 1) MPH MHA PHD FRANZCO is a medical retina specialist and Professor of Ophthalmology at the University of Sydney. She is a consultant medical retina specialist at Royal North Shore and Sydney Eye Hospital. Her leadership roles include Co-Chair of the RANZCO Diabetic Retinopathy Screening Working Group, Deputy Director of Clinical Trials at the Save Sight Institute; Medical retina section editor for Clinical and Experimental Ophthalmology, and chair of the Australian Vision Research advisory committee.
References
- International Diabetes Federation. Diabetes Atlas. Published online 2024. Available at diabetesatlas.org [accessed Apr 2026].
- Pearce I, Simó R, Evans M, et al. Association between diabetic eye disease and other complications of diabetes: implications for care. A systematic review. Diabetes Obes Metab. 2019;21(3):467-478. doi: 10.1111/dom.13550.
- Pedro RA, Ramon SA, Isabel MM, et al. Prevalence and relationship between diabetic retinopathy and nephropathy, and its risk factors in the North-East of Spain, a population-based study. Ophthalmic Epidemiol. 2010;17(4):251-265. doi: 10.3109/09286586.2010.498661.
- Huang YC, Shen FC, Wu PH, et al. Dissecting the relationship between heart failure and diabetic retinopathy severity in patients with diabetes and chronic kidney disease: an observational cohort study. Sci Rep. 2025;15(1):24346. doi: 10.1038/s41598-025-04523-1.
- Zinman B, Wanner C, Lachin JM, et al., and MPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117-2128. doi: 10.1056/NEJMoa1504720.
- Control D, Group CTR, others. Early worsening of diabetic retinopathy in the Diabetes Control and Complications Trial. Arch Ophthalmol. 1998;116(7):874-886. doi: 10.1001/archopht.116.7.874.
- Husain M, Birkenfeld AL, Bain SC, et al.; PIONEER 6 Investigators. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-851. doi: 10.1056/NEJMoa1901118.
- Marso SP, Bain SC, Vilsbøll T, et al. SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. doi: 10.1056/NEJMoa1607141.
- Chen KY, Chan HC, Chan CM. Does semaglutide increase the risk of non-arteritic anterior ischemic optic neuropathy? A systematic review and meta-analysis of emerging evidence. Asia-Pac J Ophthalmol. Published online 2025:100245. doi: 10.1016/j.apjo.2025.100245.
- World Health Organization. The use of semaglutide medicines and risk of non-arteritic anterior ischemic optic neuropathy (NAION). June 27, 2025. Available at: who.int/news/item/27-06-2025-27-06-2025-semaglutide-medicines-naion [accessed April 2026].
- Wells JA, Glassman AR, Beck RW, et al.; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123(6):1351-1359. doi: 10.1016/j.ophtha.2016.02.022.
- Wykoff CC, Abreu F, Tadayoni R, et al.; YOSEMITE and RHINE Investigators. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. The Lancet. 2022;399(10326):741-755. doi: 10.1016/S0140-6736(22)00018-6.
- Brown DM, Boyer DS, Sivaprasad S, et al.; PHOTON Investigators. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. The Lancet. 2024;403(10432):1153-1163. doi: 10.1016/S0140-6736(23)02577-1.
- Do DV, Wykoff CC, Sivaprasad S, et al. Intravitreal aflibercept 8 mg for diabetic macular edema: ninety-six-week results from the randomized Phase 2/3 PHOTON trial. Ophthalmology. 2026 May;133(5):577-588. doi: 10.1016/j.ophtha.2025.10.028.
- Chaudhary V, Guymer R, Singh RP, et al. Real-world evidence for faricimab in neovascular age-related macular degeneration and diabetic macular edema: a scoping review. Ophthalmol Sci. 2025;5(4):100744. doi: 10.1016/j.xops.2025.100744.
- Bressler SB, Odia I, Melia M, et al. Changes in diabetic retinopathy severity when treating diabetic macular edema with ranibizumab: DRCR. net protocol I 5-year report. Retina. 2018;38(10):1896-1904. doi: 10.1097/IAE.0000000000002302.
- Lois N, Campbell C, Clarke M, et al.; DIAMONDS Study Group. Diabetic macular edema and diode subthreshold micropulse laser. Ophthalmology. 2023;130(1):14-27. doi: 10.1016/j.ophtha.2022.08.012.
- Network WC for the DRCR, Gross JG, Glassman AR, Beck RW, et al. Panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2015;314(20):2137-2146. doi: 10.1001/jama.2015.15217.
- Gross JG, Glassman AR, Beck RW, et al.; Diabetic Retinopathy Clinical Research Network. Five-year outcomes of panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA Ophthalmol. 2018;136(10):1138-1148. doi: 10.1001/jamaophthalmol.2018.3255.
- Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study Report no. 4. The Early Treatment Diabetic Retinopathy Study Research Group. Int Ophthalmol Clin. 1987 Winter;27(4):265-72. doi: 10.1097/00004397-198702740-00006.
- Antoszyk AN, Glassman AR, Sun JK, et al.; DRCR Retina Network. Effect of intravitreous aflibercept vs vitrectomy with panretinal photocoagulation on visual acuity in patients with vitreous hemorrhage from proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2020;324(23):2383-2395. doi: 10.1001/jama.2020.23027.
- Khanani AM, Campochiaro PA, Malhotra V, et al. Continuous ranibizumab via port delivery system vs monthly ranibizumab for treatment of diabetic macular edema: the pagoda randomized clinical trial. JAMA Ophthalmol. 2025;143(4):326-335. doi: 10.1001/jamaophthalmol.2025.0006.
- Roche. FDA Approves Roche’s Susvimo as the First and Only Continuous Delivery Treatment for the Leading Cause of Diabetes-Related Blindness. 2025. Available at: roche.com/media/releases/med-cor-2025-02-04 [accessed March 2026].
- Pieramici DJ, Awh CC, Latkany P, et al. Port delivery system with ranibizumab vs monitoring in nonproliferative diabetic retinopathy without macular edema: The pavilion randomized clinical trial. JAMA Ophthalmol. 2025;143(4):317-325. doi: 10.1001/jamaophthalmol.2025.0001.
- Roche. FDA approves Roche’s Susvimo for diabetic retinopathy. Published online May 22, 2025. Available at: roche.com/media/releases/med-cor-2025-05-22 [accessed March 2026].
- Sharma A, Parachuri N, Bandello F, et al. The port delivery system with ranibizumab—journey of mitigating vitreous hemorrhage. Eye. 2022;36(3):488-489. doi: 10.1038/s41433-021-01830-5.
- Yang JY, Goldberg D, Sobrin L. Interleukin-6 and macular edema: a review of outcomes with inhibition. Int J Mol Sci. 2023;24(5):4676. doi: 10.3390/ijms24054676.
- Saeed O, Sheth, VS. The promise of TKIs. Retin Physician. 2025;22(3). Available at: digital.retinalphysician.com/articles/the-promise-of-tkis [accessed February 2026].
- Charters L. HELIOS trial 1-year results assess implant for treatment of non-proliferative diabetic retinopathy. Ophthalmol Times. 27 January 2025. Available at: europe.ophthalmologytimes.com/view/helios-trial-1-year-results-assess-implant-for-treatment-of-non-proliferative-diabetic-retinopathy [accessed February 2026].
- Zhelev Z, Peters J, Hyde C, et al. Test accuracy of artificial intelligence-based grading of fundus images in diabetic retinopathy screening: a systematic review. J Med Screen. 2023;30(3):97-112. doi: 10.1177/09691413221144382.